Continuing from Part I.
If Daniel Moerman, PhD is correct and the subjective improvement is what is important, then we should ignore this chart, because this chart demonstrates objective improvement.t[1] Objective improvement is what is real.
–
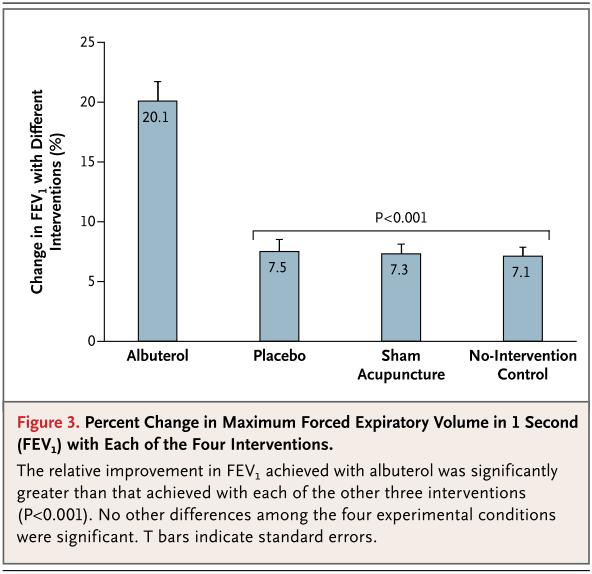
Image credit.[2]
–
If Daniel Moerman, PhD is correct and the subjective improvement is what is important, then we should pay attention to the following chart of subjective improvement. Subjective improvement is what the patient thinks is real, even if reality does not agree.
When we go to a magic show and see a woman being cut in half, we are experiencing subjective reality. The objective reality is that the woman was never really cut in half, even though our subjective experience is that she has been cut in half.
We have been tricked.
–

Click on the image to make it larger.
–
If Daniel Moerman, PhD is correct and the subjective improvement is what is important, then would it be better to give asthma patients a sedative, rather than a placebo?
Looking at that graph of subjective improvement, I suspect that with the right titration of a sedative I could produce much better subjective reports of improvement by giving an active sedative, rather than by giving albuterol, placebo albuterol, acupuncture, sham acupuncture, or any other alternative medicine treatment or the sham version of an alternative medicine treatment (as if the sham version of a sham treatment makes any difference).
–
Roughly 50% improvement in subjective assessment?
That’s nothing. I can probably get the improvement to 80% with a sedative alone.
Or I could use morphine.
Morphine would probably the same effect, even though it might produce a worsening of objective air flow.
But that would be unethical, wouldn’t it?
If I give a treatment that will produce a subjective improvement, but objective worsening, then I am harming the patient.
–
Similarly, the old practice of bleeding patients to the point where they stop complaining was abandoned. Should we bring it back? Get rid of those annoying patients by bleeding them to the point of submission or to the point where they never recover from that subjective improvement.
We just need to ignore objectivity and we can do whatever makes the patient feel better.
–

–
Footnotes:
–
[1] Meaningful placebos–controlling the uncontrollable.
Moerman DE.
N Engl J Med. 2011 Jul 14;365(2):171-2. No abstract available.
PMID: 21751911 [PubMed – indexed for MEDLINE]
–
[2] Active albuterol or placebo, sham acupuncture, or no intervention in asthma.
Wechsler ME, Kelley JM, Boyd IO, Dutile S, Marigowda G, Kirsch I, Israel E, Kaptchuk TJ.
N Engl J Med. 2011 Jul 14;365(2):119-26.
PMID: 21751905 [PubMed – indexed for MEDLINE]
–
Wechsler, M., Kelley, J., Boyd, I., Dutile, S., Marigowda, G., Kirsch, I., Israel, E., & Kaptchuk, T. (2011). Active Albuterol or Placebo, Sham Acupuncture, or No Intervention in Asthma New England Journal of Medicine, 365 (2), 119-126 DOI: 10.1056/NEJMoa1103319
Moerman, D. (2011). Meaningful Placebos — Controlling the Uncontrollable New England Journal of Medicine, 365 (2), 171-172 DOI: 10.1056/NEJMe1104010
.



Our job is to provide objective AND subjective relief. It is not an either or proposition. I also dispute the assertion that providing subjective relief is not beneficial to patient status. Anxiety increases oxygen demand and causes the release of all kinds of nasty intrinsic chemicals which are not conducive with good-health. For years I have treated dyspnea patients under both the “difficulty breathing” protocol and the “anxiety” protocol. Whether they are having a panic attack (I think most prehospital providers would agree that a large number of patients have some degree of psychiatric issue, diagnosed or not) or are merely anxious BECAUSE THEY CAN’T BREATHE, they are still anxious. I believe it is ethical and medically proper to treat the bronchoconstriction AND the anxiety. Why wouldn’t we want to improve the patient’s physical and emotional simultaneously if we have the capacity.
“If Daniel Moerman, PhD is correct and the subjective improvement is what is important,…”
Sorry, but any improvement in subjective scores must translate into objective, functional, real world gains. Improving scores on subjective measures, without an accompanying objective improvement, is meaningless manipulation of test taking behaviour.
Teeks, I think you may have missed the sarcasm coming from Rogue. I am pretty sure the implication was not to abandon procedures and medications that provide measurable, physical relief to the patient. I believe the intent was to mock the fact that someone would waste time and energy measuring and reporting subjective relief in the first place. I stand by my post that if we can provide subjective relief WITH objective relief, then we are caring for the whole patient and not just attacking the signs and symptoms. Compassionate caregivers consider the patient’s emotional well-being in the course of care and do not merely treat the patient’s physical ailments.
Also, since these were treatment studies, I am not sure how you would end up with manipulation of test-taking behavior. The “test” in this case was relief of symptoms. I doubt someone with dyspnea cares much how their behavior affects a study. They just want relief! The smart ones would probably tell you they expect objective relief, but they would settle for the subjective relief because THAT is what makes them feel better. It’s sort of like making cough syrup taste good. The nasty tasting stuff may give you objective relief, but if you can add a little sweetener and some flavoring, you can achieve the objective while sparing the patient the awful aftertaste of the just as beneficial but heinous medicine that tastes like, well, medicine.
Thought #1: How many of our patients call us for relief of objective complaints? Certainly part of our job is to catch and provide a path to the treatment of dangerous “objective” problems, but strictly speaking, that’s not usually why they called us. Note we call it a “chief complaint,” not a “chief pathology,” even if many of us have started conflating the two. My arm hurts. I feel bad. I’m dizzy.
Thought #2: If we grant that it’s important to correct things that can lead to additional morbidity and mortality, surely you do not OPPOSE making people feel better.
Your analysis is incomplete because it does not include the side effects and cautions associated with albuterol use compared to placebo, sham acupuncture and acupuncture.
After a thorough analysis the pharmaceutical may or may not be the best choice but until BOTH the pros and the cons of all the treatments and approaches are tallied and compared, making a decision is premature.
Here is one tally of the adverse effects of several forms of albuterol: http://www.rxlist.com/proventil-drug.htm
medskep,
I analyzed the editorial and the podcast comments of Daniel Moerman, PhD. If he had compared the adverse event rate of the placebo treatments to the adverse event rate of the albuterol, then there would be a reason to claim that my analysis was incomplete. He did not address this, so I did not address this.
–
I agree that any treatment should have all of the side effects considered before use.
The active drug will have side effects, but so will the placebo. The placebo side effects are referred to as nocebo effects. Sometimes the placebo will have worse side effects than the active drug. The list of side effects does not mean that they were caused by the drug, but that they have been reported in association with the use of the drug.
With an active drug, some of the side effects will be due to the drug and some will not.
With a placebo, some of the side effects will be nocebo effects and some will only be coincidence.
Some of the side effects will be unrelated with both the active drug and with the placebo
I changed the link. It still goes to the same place, but I would rather have people able to see where they are going, since there are so many scam sites that bit.ly links might direct them to.
A better site is –
PROAIR (albuterol sulfate) aerosol, metered
[Teva Respiratory, LLC]
DailyMed
FDA Drug Label
http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=23099
Catecholamines will be expected to produce tachycardia and/or headache at a greater rate than placebo will. On the other hand, the drug companies are constantly working to decrease the side effects of these drugs. Aminophylline and epinephrine were used routinely for asthma several decades ago. They produce much more frequent tachycardia and/or headache.
The rate of tachycardia was about 5% with albuterol. the rate of headache was about 10% with albuterol. Patients experiencing those side effects may decide to use a different treatment, or they may try albuterol again and not experience side effects, or they may decide that the side effects are a small price to pay for the ability to really improve their breathing.
With more severe asthma, this choice is much less important. Life threatening asthma that can be reversed with a drug that causes tachycardia and/or headache? Save my life and I will put up with the tachycardia and/or the headache. Still this seems to affect only a small portion of the patients.
Consider the same patient with life threatening asthma who decides to use acupuncture, or sham acupuncture, or a placebo inhaler. Will any of those treatments reverse the life threatening asthma? No.
Will the albuterol reverse the life threatening asthma? Albuterol is the initial treatment for many patients. If that does not work, then more potent drugs with probably more pronounced and more frequent side effects will be used. I have never had a patient tell me that the side effects are to severe for any of these treatments.
Does albuterol have side effects?
Yes.
Do placebos have side effects?
Yes.
Is your analysis of the side effects incomplete because you did not mention the side effects that are observed with placebos?
.
.
Thank you for your thoughtful reply and for the link you provided.
In life threatening situations using a drug with more severe side effects is a more reasonable choice than using a less effective approach with fewer side effects.
Problem is that in many non-life threatening situations drugs with more severe side effects are used when a milder approach with fewer or less intense side effects will do.
This is a good reason to have a variety of approaches to use even when by some measures one is clearly more powerful.
medskep,
Thank you.
Yes.
Benign neglect is sometimes the best treatment.
However, the problems with medicine do not mean that there is any reason to use any alternative medicine.
If alternative medicine could demonstrate that it works, alternative medicine would be called medicine.
We rush to use treatments, even when there is no evidence of efficacy.
We should limit ourselves to treatments that have been demonstrated to be better than placebo and we should make sure that we provide patients with full information about the potential effects and potential side effects of any treatment.
.