In the comments to The Danger of ROSC – Return Of Spontaneous Circulation is the following from Walt Trachim of Living in Manch Vegas.
–
I have a question, though. What is the actual pathophysiology that causes the damage to brain tissue?
If it were obvious that this would cause brain damage, there would not be people supporting the use of epinephrine. I do not see this as any kind of conspiracy, just the usual overestimation of our abilities that humans are so good at.
This is one of the reasons I try to avoid the Why explanations. We take the limited information and extrapolate from that to what happens in a much more general situation. The one thing we should count on is that the explanation is wrong.
As a species we want to know Why.
As people delivering patient care, we need to ignore the question Why and limit ourselves to Does it work?
Eventually we will have a much better understanding of the reasons Why, but if we understood that, we would not need to study treatments. We could just learn the pathophysiology and the answer would be clear. The many abandoned treatments make it very clear that our understanding of CPR is nowhere near good enough for that.
I don’t know Why. I could guess, but guessing (almost all of the recent explanations of Why the body does something) is just a way to come up with errors to be corrected later. I make errors, but I try to limit the frequency and significance of my errors.
We know that more people treated with epinephrine will die in the hospital.
We know that more people treated with epinephrine will have severe brain damage.
Do we need to know Why before we stop using epinephrine?
If I put my hand in a fire, do I need to understand the mechanisms of damage before I decide to pull my hand out of the fire?
–
Assuming that ROSC does happen, how does the Epinephrine that is given (and has a relatively short half-life) cause the kind of tissue damage that you’re talking about? Does it cause furthering hypoxia? Is it chemical? I’m trying to understand this a little better because I’m not sure why the relatively small doses that we use in the field could do the type of damage you describe.
See above for the Why explanations.
relatively small doses?
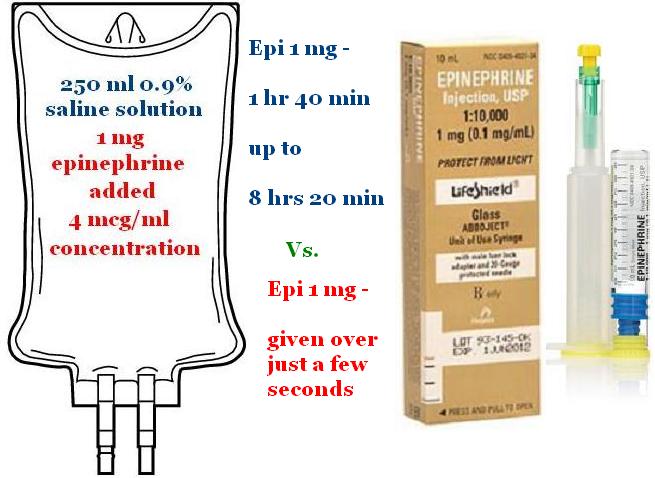
Epinephrine in live humans is given at 2 μg/minute to 10 μg/minute.
Epinephrine in dead humans is given at 1,000 μg all at once.
2 – 10 vs 1,000.
That is a huge difference.
There is nothing small about the epinephrine doses we give in cardiac arrest.
–
–
And this brings another question to mind: what about when Epinephrine is being used in a non-cardiac arrest situation? Specifically, if you’re dealing with someone who is in Anaphylaxis and is being given Epi in the 1:1000 concentration (albeit at a lower dose) for bronchodilation and vasoconstriction, would the concerns you’re talking about regarding tissue damage still apply? Based on the circumstances you’re detailing in your research and analysis, I’m inclined to think they would, but I’m definitely interested to read your thoughts on this.
We do give 300 μg IM (IntraMuscular) to anaphylaxis patients, but IM absorption is slower than IV and there is evidence that epinephrine is effective at preventing death in these patients.
What is the right dose of epinephrine for someone who is probably having a heart attack?
The most common cause of cardiac arrest is heart attack, so we should assume that these patients are having heart attacks.
I think that the right dose of epinephrine for a patient having a heart attack is zero μg.
–
I’m asking these questions for a very simple reason: you made me think. You’re really good at that, by the way. And, as I said, I want to understand the “why” more clearly. And since I’ve been a full-time student again, my brain has been engaged much more than it usually is.
Merry Christmas, and thanks for putting up with pestilent questions. 🙂
These are not pestilent questions. Asking questions is the way we learn. When we stop asking questions, it will not be because we have the answers to everything, but because we have lost our curiosity.
We need to accept that almost always we do not know Why.
Why does gravity pull us toward massive objects?
Why does the Sun work by nuclear fusion?
Why are there mosquitoes?
Why do we die?
The Why questions are great for coming up with hypotheses, but they will also keep you decades behind in treating patients.
An empirical approach can be less satisfying, but only if we insist on knowing Why.
–
See also –
How did this happen? – Research
.



Another excellent article. I suppose it’s my earlier career in chemistry that makes me put up a defense of “why?”
I absolutely agree that pre-hospital EMS is not the place to look for “why”, for the reason you mention in your research article: we can never adequately control the variables well enough. Research in the field (and all empirical/epidemiological research) tends to be of the “works or doesn’t work” type. As you pointed out, it would tell us that a 1mg bolus of epi doesn’t work. Looking at “why” can tell us if the problem is the drug, dose, delivery, AND give ideas of possible alternatives ( e.g. Infusion of vasopressors).
I admit that I don’t know how these experiments would be done in practical terms. At least smelly chemicals don’t have relatives who can sue or, even worse, be present begging the researcher to “do everything to save them”.
Mike,
There is nothing wrong with curiosity, but we should be realistic in our expectations of what we know about medicine.
–
We tend to make the mistake of assuming that a dead patient (a low metabolic state) needs more drug than a live patient. The opposite is more likely to be true.
We assume that the drugs we give get into the central circulation because we want them to be there. We do not consider that the drugs we give sit in the peripheral circulation until after the heart starts to improve the circulation to the extremities – and then moves those drugs, at doses that would never be given intentionally to a live human, to the central circulation. How many post-epinephrine heart rates under 100 do we see?
How long does it take for that toxicity to go away?
How does that help the heart?
How does that help the brain?
–
Eventually we will have large enough outcomes studies of epinephrine.
We can expect that the results will make the ACLS permanent recommendation to give epinephrine to every cardiac arrest patient will look really bad, but like a company facing bankruptcy, gambling everything on some Hail Mary magic is to be expected as the evidence against epinephrine grows.
Some people will claim that the results of the recent Australian study provide some defense of epinephrine –
Anyone looking at 4% survival as some kind of justification for anything should not be making patient care decisions.
The study from Norway had much better results.
6% of the patients receiving adrenaline (epinephrine) were alive one year later.
12% of the patients not receiving adrenaline (epinephrine) were alive one year later.
Outcome when adrenaline (epinephrine) was actually given vs. not given – post hoc analysis of a randomized clinical trial.
Olasveengen TM, Wik L, Sunde K, Steen PA.
Resuscitation. 2011 Nov 22. [Epub ahead of print]
PMID: 22115931 [PubMed – as supplied by publisher]
Defenders of epinephrine will point to the higher percentage of patients discharged, but ignore the unacceptably low rate of survival to discharge. This is not the way medicine makes progress.
Does Epinephrine Improve Survival from Cardiac Arrest
.