–
Is the harm from furosemide (Lasix – frusemide in Commonwealth countries) anything new?
This study is looking at the effects of furosemide in patients with chronic CHF (Congestive Heart Failure), not acute exacerbations of CHF. This should have led to studies of the effects of furosemide on acute CHF. After all, in 1985 everyone seems to have been using furosemide for acute CHF.
Our clinical observation of what appeared to be acute worsening of symptoms after intravenous furosemide administration in some patients with severe heart failure led us to study the sequential hemodynamic and neurohumoral responses in a series of such patients.[1]
We have seen patients get worse. It is 1985. We are not the first to study this, but emergency medicine and EMS will not really cut back on the use of furosemide for acute CHF until after 2000 – more than a decade and a half.
All patients had clinical evidence of congestive heart failure for at least 6 months and were hospitalized for heart failure. No patient had frank pulmonary edema. The average ejection fraction, as measured by radionuclide angiography in 14 patients, was 22 ± 5% (SD).[1]
Each patient was on a sodium-restricted diet, and all had symptoms typical of New York Heart Association class III to IV.[1]
These were sick patients at baseline. It is not clear if these patients were already in the hospital for treatment of CHF or if they were recruited as outpatients. No patients had heart attacks within the previous 4 months.
Digitalis and diuretics were used chronically by all patients, but none had used vasodilator therapy for at least 72 hours before the study. Most patients were receiving chronic furosemide therapy, but the usual morning dose was withheld until the study (usually midmorning).[1]
Is IV (IntraVenous) furosemide worse than oral furosemide?
When treating acute CHF, do we really care?
Each patient then received an average dose of 1.3 ± 0.6 mg/kg body weight of furosemide given over 1 to 2 minutes.[1]
For a 70 kg patient, that would be 91 mg ± 42 mg (between 49 mg and 133 mg [between 0.7 mg/kg and 1.9 mg/kg]) over one to two minutes. Not a huge dose, but not a tiny dose, either.
Two patients became noticeably shorter of breath by 10 to 20 minutes after furosemide administration.[1]
If the patient is healthy enough for us to give them a drug that makes them sicker, are they surviving their illness or are they just surviving our abuse?

Immediately increased heart rate. How much worse would it become if the patient had acute pulmonary edema?

Immediately decreased stroke volume. How much worse would it become if the patient had acute pulmonary edema?
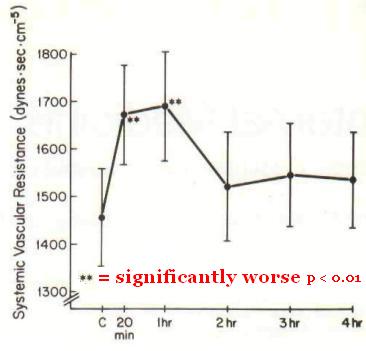
Immediately increased systemic vascular resistance. How much worse would it become if the patient had acute pulmonary edema?
If the heart rate gets worse, the stroke volume gets worse, and the systemic vascular resistance gets worse, then we expect the blood pressure to get worse. Is the blood pressure going to get worse by dropping or by increasing?

The most effective medical treatment for acute pulmonary edema is vasodilators – especially high-dose NTG (NiTroGlycerin – GTN GlycerylTriNitrate in Commonwealth countries).
Furosemide is doing exactly the opposite of what we want it to do.
–
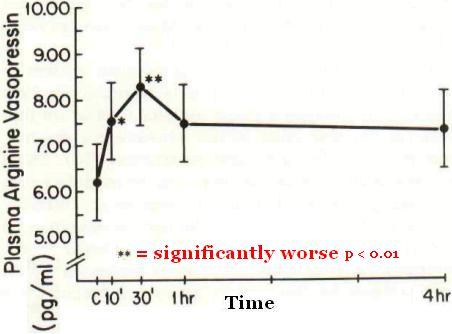
An increase in plasma arginine vasopressin levels after furosemide administration is also a new finding.[1]
This is not what we want.
–

Activation of the sympathetic nervous system by intravenous furosemide treatment in patients with congestive heart failure is a new finding.[1]
This is not what we want.
The use of intravenous furosemide in patients with chronic congestive heart failure, although well established, can promote further clinical hemodynamic deterioration during the first 20 minutes.[1]
Traditional, but harmful.
In other words – Standard Of Care.
This deterioration may go largely unnoticed because such patients often are already dyspneic and show clinical improvement over the next hour.[1]
Maybe we need to pay more attention to what is going on with our patients, rather than paying attention to killer traditions.
We could get similar results with a bolus of epinephrine, but we usually wait until the patient is dead to do that.
Maybe the only reason we don’t give furosemide in cardiac arrest is that we are afraid that it might make the patient pee.
These patients were not having acute attacks of CHF before receiving furosemide.
These patients got a lot worse before they returned to their baseline.
Is there any reason to believe that the furosemide behaves any better when the CHF patient is already short of breath and his lungs are filling with fluid?
The furosemide is supposed to work on the kidneys, but acute CHF patients have poor circulation to the kidneys, so even that is not likely to do anything until after the patient is much better.
Other posts on furosemide (Lasix).
–
Footnotes:
–
[1] Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart failure. Activation of the neurohumoral axis.
Francis GS, Siegel RM, Goldsmith SR, Olivari MT, Levine TB, Cohn JN.
Ann Intern Med. 1985 Jul;103(1):1-6.
PMID: 2860833 [PubMed – indexed for MEDLINE]
–
Francis GS, Siegel RM, Goldsmith SR, Olivari MT, Levine TB, & Cohn JN (1985). Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart failure. Activation of the neurohumoral axis. Annals of internal medicine, 103 (1), 1-6 PMID: 2860833
.



Frusemide. We call it Frusemide.
Cannulator,
I added this to the initial information – furosemide (Lasix – frusemide in Commonwealth countries).
.
Cheers. You know how easily muddled we get ; )
As a general principle I adhere to the is-this-really-necessary-rule of thumb. I wrote about that here: http://contusio-cordis.blogspot.no/2011/02/house-of-god.html