
Last week on EMS Office Hours, Jim Hoffman, Josh Knapp, and Dave Brenner discussed a variety of topics before I got on the show. We ended up discussing a question Josh had posted on the WANTYNU Facebook page.
EMS Volunteers, Patient Stress and 200,000
I do not have a link to the original question, but it was along the lines of If you are 99% sure that your patient is having a heart attack, do you tell the patient?
My original comment was along the lines of
1. How did I develop so much certainty about this actually being a heart attack?
2. What is the benefit of telling the patient You are having a heart attack?
1.
A. Do we track all of our heart attack patients and compare their final diagnoses with our diagnoses?
Would only STEMIs (ST segment Elevation Myocardial Infarctions) be considered for the You are having a heart attack, with 99% accuracy claim?
Does we have the statistics to back up that claim?
Are we overly confident of our diagnoses and unaware of the difference between our accuracy and reality?
Even if we do track our precision (when we state that it is a heart attack, it truly is a heart attack), do we assume that means that we avoid false negatives(when we do not state that it is a heart attack, there is no heart attack)?
Do we track false negatives?
How do we know if we miss false negatives?
How does awareness of these false negatives affect our confidence in claiming You are having a heart attack?
Do our misses count?
Is it a miss, if the machine analysis states ***STEMI***, we disagree, but it turns out to be a STEMI?
Is it a miss, if the machine analysis does not state ***STEMI***, we disagree, and it turns out to not be a STEMI?
Is it a miss, if the machine analysis does not state ***STEMI***, we disagree, but it turns out to be a STEMI? The machine was wrong, but we were right.
All of these affect our diagnosis of STEMI, but how much do we pay attention to any of them?
Is the excuse, Most doctors would have missed that, a valid excuse? We are wrong, but we are as wrong as another group of people would be expected to be.
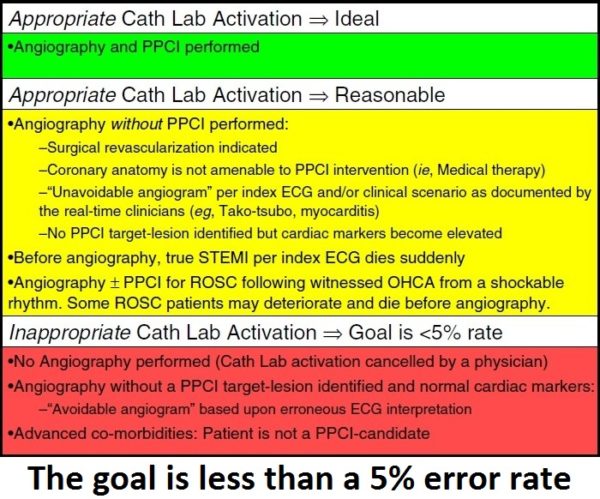
If the goal is to be wrong less than 5% of the time, what evidence do we have that we are wrong less than 1% of the time?
In summary, broad awareness should exist regarding evidence-based triggers for appropriate Cath Lab activation. A diverse group of frontline clinicians making these time-pressured decisions need a comprehensive list of precise criteria, because not all “acute MIs” have classic ST-elevation on ECG (eg, STEMI-equivalents and certain OCHA scenarios), not all ST-elevation patterns represent “true STEMI” (ie, STE-mimics), and some “true STEMI” patients are not reasonable candidates for an aggressive treatment strategy involving PPCI. Optimal ECG interpretation proficiency by all clinicians in identifying both classic STEMI and STEMI-equivalents constitutes a major cornerstone of ongoing efforts to maximize STEMI system efficiency.[1]
And the most important question may be How much do we know about what we don’t know?
Am I 99% certain, or just convincing myself that I am much more certain than I have any right to claim?
Why should we assume that we do not need to know our limitations?
Also see Tom Bouthillet’s slides from his presentation –
STEMI Mimics and STEMI Equivalents
EMS 12 Lead
Slide presentation.
–
Footnotes:
–
[1] Appropriate cardiac cath lab activation: optimizing electrocardiogram interpretation and clinical decision-making for acute ST-elevation myocardial infarction.
Rokos IC, French WJ, Mattu A, Nichol G, Farkouh ME, Reiffel J, Stone GW.
Am Heart J. 2010 Dec;160(6):995-1003, 1003.e1-8. doi: 10.1016/j.ahj.2010.08.011. Review.
PMID:21146650[PubMed – indexed for MEDLINE]
Free Full Text from Am Heart J.
.



Well, EMTs and paramedics can’t diagnose, so that sort of simplifies the issue…
All kidding aside, I think many physicians go out of there way to avoid projecting false certainty. Abdominal pain without a discernible cause is diagnosed as “abdominal pain,” and so on. There is a time and place for looking a patient square in the eyes and saying “You have XYZ, and this is what’s going to happen,” but most of the time it’s acceptable, preferable even, to express some uncertainty.
Was there some sort of conflict or controversy that prompted this set of questions?
If I’m going to start an IV, administer multiple medications, and rush you off to a cath lab L&S, I think I owe you the courtesy of explaining my thinking. I’m not going to tell you I’m certain, but patients deserve some
explanation of our “working diagnosis” and their course of treatment. How else can patients give informed consent?