
Image from Bloomberg.com.
0.15 mg (0.15 ml of 1 mg/ml epinephrine) for a child.
0.3 mg (0.3 ml of 1 mg/ml epinephrine) for an adult.
Inject deep into the side of the thigh.
This should not be complicated, but . . . .
Paramedics have generally been able to give epinephrine injections for anaphylaxis in Illinois and elsewhere. As of January 1, 2017, basic EMTs (Emergency Medical Technicians) in Illinois, who have been able to use the EpiPen autoinjector, will be able to give epinephrine injections the same way paramedics give epinephrine for anaphylaxis.[1],[2]
Why? The cost of the autoinjector has increased from around $100 to around $600 since 2007, when Mylan bought the EpiPen as part of a group of products from Merck. During that time, the packaging has gone from a single EpiPen to two EpiPens, so that may be one part of the increase.
The EpiPen, which is currently only made by Mylan, used to have competition from Sanofi. On October 30, 2015, Sanofi recalled their Auvi-Q autoinjectors due to the possibility of dosage inaccuracies.[3] Some people are claiming that the increase in cost is due to the withdrawal of this competitor from the market, but I was able to locate two other competitors in the US, so there is competition.
Explanations exist; they have existed for all time; there is always a well-known solution to every human problem — neat, plausible, and wrong. H.L. Mencken.
If only the Sanofi recall caused the price increase, the price would not have been increasing for the past 10 years, but only for the past 10 months. Here is a graph of the price increase before the Sanofi recall.
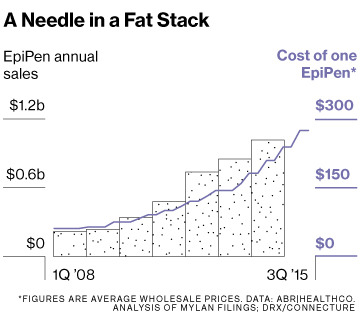
Graph from September 2015 – before the Sanofi recall – from Bloomberg.com.[4]
There are other competitors out there. Adrenaclick by Amedra Pharmaceuticals LLC,[5] and epinephrine injection, USP auto-injector by Lineage Therapeutics Inc.[6] – both located in Horsham, PA and the web sites have the same design, so they may be manufactured in the same facility.
The problems with having basic EMTs giving epinephrine injections are that the education has to be very good and the oversight has to be aggressive. As with naloxone (Narcan), doctors, nurses, and paramedics often give the drug inappropriately, so we know that there is a lot of potential for error.
The closest children’s hospital only uses autoinjectors, because they do not allow the nurses to draw up epinephrine for anaphylaxis. They probably do not allow the doctors to either, but I did not ask.
How bad are doctors at diagnosing and treating anaphylaxis?
Senior house officers (SHOs) (n=78) at the start of their accident and emergency (A&E) post were given an anonymous five case history questionnaire, containing one case of true anaphylaxis, and asked to complete the medication they would prescribe. In the case of anaphylaxis, 100% would administer adrenaline (epinephrine) but 55% would do so by the incorrect route. In the remaining cases, 10%–56% would be prepared to administer adrenaline inappropriately. Only 5% were able to indicate the correct route and dose of adrenaline according to Resuscitation Council guidelines (UK). This has implications for training as the survey took place before the start of the A&E posting. Anaphylaxis is over-diagnosed and poorly treated despite Resuscitation Council guidelines.[7]
That was in 2002. Have things improved?
RESULTS:
68 of 107 (64%) junior doctors completed the questionnaire. All recognised the need for adrenaline in anaphylaxis, but only 74% selected the correct intramuscular route, and 34% the correct route and dose. 82% of junior doctors would inappropriately give adrenaline to the patient who had inhaled a foreign body (case 2). A higher percentage of the 2013 cohort indicated the correct route and dose of adrenaline in anaphylaxis than their 2002 colleagues. However, a greater percentage also selected adrenaline treatment inappropriately in non-anaphylactic case scenarios.CONCLUSIONS:
Despite updated guidelines, junior doctors continue to have poor knowledge about the recognition and management of anaphylaxis, with some still considering inappropriate intravenous adrenaline. More effort should be given to the recognition of anaphylaxis in early medical training.[8]
Other research on doctors shows similar inability to come up with the right diagnosis, the right dose, and/or the right route of administration.[9],[10],[11] There are more. My anecdotal experience is that this is also a problem in the US with experienced paramedics and experienced physicians.
What about the King County epinephrine kit for basic EMTs?

Image from the Seattle Times.
With training, EMTs in the program have learned to administer epinephrine efficiently and safely, he said. An EpiPen takes about 45 seconds to administer, start to finish. With the vial and syringe, it’s about 2 minutes, Duren said.[12]
As a paramedic, I am not going to be much faster.
“That sounds reasonable,” Reiter said. “For all but the most severe cases of anaphylaxis, a one-minute time lag is unlikely to make a difference.”[12]
The article suggests that King County is tracking their results carefully, which does not appear to be the case for EMS systems that have first responders giving naloxone. I would still like to see something published in a peer reviewed journal.
–
Footnotes:
–
[1] New state law will allow EMTs to inject epinephrine
Dan Petrella
The Southern Springfield Bureau
The Southern Illinoisan
Updated 22 hrs ago
Article
–
[2] New Ill. law to allow all EMTs to use syringes to administer epinephrine – The new law will allow EMTs with basic-level training to use a syringe to administer epinephrine
By EMS1 Staff
EMS1.com
Yesterday at 12:59 PM
Article
–
[3] UPDATED: Sanofi US Issues Voluntary Nationwide Recall of All Auvi-Q® Due to Potential Inaccurate Dosage Delivery
FDA (Food and Drug Administration – US)
For Immediate Release
October 30, 2015
Recall notice
–
[4] How Marketing Turned the EpiPen Into a Billion-Dollar Business – Mylan’s marketing turned the allergy device into a must-have.
Cynthia Koons and Robert Langreth
Bloomberg Businessweek
September 23, 2015 — 10:00 AM EDT
Article
–
[5] How to use Adrenaclick (epinephrine injection, USP auto-injector)
Adrenaclick by Amedra Pharmaceuticals LLC, Horsham, PA
Web site
–
[6] epinephrine injection, USP auto-injector
Lineage Therapeutics Inc., Horsham, PA
Web site
–
[7] Proposed use of adrenaline (epinephrine) in anaphylaxis and related conditions: a study of senior house officers starting accident and emergency posts.
Gompels LL, Bethune C, Johnston SL, Gompels MM.
Postgrad Med J. 2002 Jul;78(921):416-8.
PMID: 12151658
Free Full Text from PubMed Central.
–
[8] Correct recognition and management of anaphylaxis: not much change over a decade.
Plumb B, Bright P, Gompels MM, Unsworth DJ.
Postgrad Med J. 2015 Jan;91(1071):3-7. doi: 10.1136/postgradmedj-2013-132181.
PMID: 25573132
Free Full Text from Postgrad Med J.
–
[9] Survey of the use of epinephrine (adrenaline) for anaphylaxis by junior hospital doctors.
Jose R, Clesham GJ.
Postgrad Med J. 2007 Sep;83(983):610-1.
PMID: 17823230
Free Full Text from PubMed Central
–
[10] Anaphylaxis: lack of hospital doctors’ knowledge of adrenaline (epinephrine) administration in adults could endanger patients’ safety.
Droste J, Narayan N.
Eur Ann Allergy Clin Immunol. 2012 Jun;44(3):122-7.
PMID: 22905594
–
[11] Treatment of a simulated child with anaphylaxis: an in situ two-arm study.
O’Leary FM, Hokin B, Enright K, Campbell DE.
J Paediatr Child Health. 2013 Jul;49(7):541-7. doi: 10.1111/jpc.12276. Epub 2013 Jun 12.
PMID: 23758136
Free Full Text from J Paediatr Child Health.
RESULTS:
Fifty-six junior medical staff participated (90% participation rate). Only 50% of participants administered adrenaline in scenarios of definite anaphylaxis. Adrenaline was more likely to be administered if the scenario included hypotension, where the junior medical officer had previous formal resuscitation training (Advanced Paediatric Life Support) and by medical officers with more years of training.CONCLUSION:
Anaphylaxis is a life-threatening presentation and requires prompt recognition and appropriate adrenaline administration. Junior medical staff may require more emphasis on recognition and prompt adrenaline administration in both undergraduate and in hospital training and education. Simulated scenarios may provide a platform to deliver this training to ultimately improve patient care.
–
[12] King County drops EpiPen for cheaper kit with same drug
By JoNel Aleccia
Seattle Times health reporter
Originally published January 14, 2015 at 10:05 pm
Updated January 15, 2015 at 7:00 pm
Seattle Times
Article
.


Subscribe to RogueMedic.com