Is prehospital use of NTG (NiTroGlycerin; GTN GlycerylTriNitrate in Commonwealth countries) safe for treating prehospital suspected STEMI (ST segment Elevation Myocardial Infarction) patients?
The evidence is limited, but does not suggest that prehospital NTG produces enough harm to discourage use in suspected STEMI. These researchers looked at the emergency department assessments of patients following prehospital NTG for suspected STEMI.
 Click on the image of the LA County protocol to make it larger.[2]
What about the 17% of suspected STEMI patients with SPB <100 mmHg who were treated with NTG?
Was medical command (California has certified MICNs [Mobile Intensive Care Nurses] providing medical command on the radio, with physicians available, as well) contacted for authorization to deviate from the protocol? If so, that is something that should be documented in the charts, which were reviewed for this paper. That information is not included in this paper. Those patients are much more interesting to me.
I do not object to using NTG to treat suspected STEMI with an SBP below 100 mmHg, but the authors seem to think that EMS should not even consider it. Do the outcomes of those patients support the approach of the authors? We do not know.
I suspect that the fears of bottoming out the blood pressure are very exaggerated, but it would be nice to have some evidence either way.
An important secondary end point was the differences between those with inferior/right ventricular STEMI, but treated with NTG.
Click on the image of the LA County protocol to make it larger.[2]
What about the 17% of suspected STEMI patients with SPB <100 mmHg who were treated with NTG?
Was medical command (California has certified MICNs [Mobile Intensive Care Nurses] providing medical command on the radio, with physicians available, as well) contacted for authorization to deviate from the protocol? If so, that is something that should be documented in the charts, which were reviewed for this paper. That information is not included in this paper. Those patients are much more interesting to me.
I do not object to using NTG to treat suspected STEMI with an SBP below 100 mmHg, but the authors seem to think that EMS should not even consider it. Do the outcomes of those patients support the approach of the authors? We do not know.
I suspect that the fears of bottoming out the blood pressure are very exaggerated, but it would be nice to have some evidence either way.
An important secondary end point was the differences between those with inferior/right ventricular STEMI, but treated with NTG.
Despite the theoretical risk, the limited retrospective studies of NTG in the prehospital setting for multiple indications suggest that the medication is safe.(10-13) However, with regard to NTG use for STEMI, the AHA International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care concluded that there was not enough evidence to determine the benefit or harm of out-of-hospital use of NTG.(14) Given the high false positive rates for STEMI identified in the field, an additional concern is that many patients treated with NTG for presumed STEMI will ultimately have an alternate etiology for their pain.(15, 16) Therefore, it is not clear that the benefits outweigh the risks of administering NTG to all patients with suspected STEMI in the field.[1]This paper helps to show the safety of prehospital NTG for suspected STEMI, providing evidence that blood pressure changes were similar in suspected STEMI patients with an SBP (Systolic Blood Pressure) of 100, or higher, regardless of whether they were treated with NTG. The study is a retrospective chart review, so we do not know why some of the patients were not treated with NTG. One reason mentioned, but not discussed, is that only 22% (96 of 440) suspected STEMI patients not treated with NTG are documented to have had pain, but there is no information on the type of pain or other cardiac symptoms of the patients. Were the paramedics avoiding treating atypical chest pain, such as pressure, heaviness, gastric discomfort, difficulty breathing, et cetera? We do not know. Was only chest pain being documented, rather than shoulder, or arm, or jaw, pain? We do not know. Did the pain resolve prior to EMS arrival? We do not know. Were the paramedics correctly recognizing when the machine interpretation of the ECGs (ElectroCardioGrams) were wrong? We do not know. The median Initial Pain Score is documented as 8, with an IQR (Inter-Quartile Range) of 5-9 for those treated with NTG. For those not treated with NTG the Initial Pain Score is documented as 0, with an IQR of 0-0. We do not know the Initial Pain Score of those who did have pain, but were not treated with NTG. All of these patients were in an IQR that was not documented in the paper. The good news is that the suspected STEMI patients not treated with NTG act as a control group, although possibly with important differences that are not discussed in the paper.
 Click on the image of the LA County protocol to make it larger.[2]
What about the 17% of suspected STEMI patients with SPB <100 mmHg who were treated with NTG?
Was medical command (California has certified MICNs [Mobile Intensive Care Nurses] providing medical command on the radio, with physicians available, as well) contacted for authorization to deviate from the protocol? If so, that is something that should be documented in the charts, which were reviewed for this paper. That information is not included in this paper. Those patients are much more interesting to me.
I do not object to using NTG to treat suspected STEMI with an SBP below 100 mmHg, but the authors seem to think that EMS should not even consider it. Do the outcomes of those patients support the approach of the authors? We do not know.
I suspect that the fears of bottoming out the blood pressure are very exaggerated, but it would be nice to have some evidence either way.
An important secondary end point was the differences between those with inferior/right ventricular STEMI, but treated with NTG.
Click on the image of the LA County protocol to make it larger.[2]
What about the 17% of suspected STEMI patients with SPB <100 mmHg who were treated with NTG?
Was medical command (California has certified MICNs [Mobile Intensive Care Nurses] providing medical command on the radio, with physicians available, as well) contacted for authorization to deviate from the protocol? If so, that is something that should be documented in the charts, which were reviewed for this paper. That information is not included in this paper. Those patients are much more interesting to me.
I do not object to using NTG to treat suspected STEMI with an SBP below 100 mmHg, but the authors seem to think that EMS should not even consider it. Do the outcomes of those patients support the approach of the authors? We do not know.
I suspect that the fears of bottoming out the blood pressure are very exaggerated, but it would be nice to have some evidence either way.
An important secondary end point was the differences between those with inferior/right ventricular STEMI, but treated with NTG.
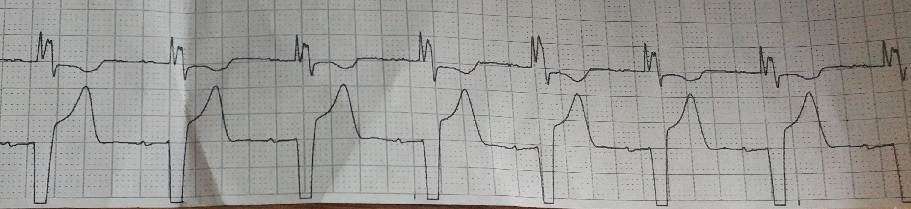
By vasodilating all blood vessels, and the venous system in particular, it causes a drop in blood pressure and preload. Thus, there is concern for precipitating hypotension in ACS involving the right ventricle.(1-3) Contraindications to the use of NTG, as outlined by the American Heart Association (AHA) Guidelines on the treatment of ACS, include right ventricular infarction.(4) This raises concern for use in inferior ST-segment elevation myocardial infarction (STEMI) in the prehospital setting, since many inferior STEMI result from proximal right coronary artery (RCA) occlusion and 50% involve the right ventricle.(3) Traditional 12-lead ECG is focused mainly on the left side of the heart and typically EMS protocols do not include acquisition of right-sided ECG leads. Further, in many systems, Basic Life Support (BLS) protocols allow for administration of NTG without differentiating the location of STEMI. There is also risk of other adverse events including bradycardia and cardiac arrest.(5-9)[1]I have aggressively promoted the use of NTG for even hypotensive CHF/ADHF (Congestive Heart Failure/Acute Decompensated Heart Failure). Many physicians are not comfortable with that, even though the available evidence shows that aggressive IV NTG doubled the survival rate for these hypotensive patients. More research is needed on the use of NTG, especially in hypotensive patients.
Further, we did not find an increased risk of hypotension among patients with proximal or mid RCA occlusions confirmed on coronary angiography. There are several possible reasons for our findings. First, while right ventricular involvement in inferior STEMI is common, hemodynamic instability is actually rare due to the right ventricle’s more favorable oxygen supply-demand ratio compared to the left heart and more extensive collateral flow.(3, 22) In addition, left heart occlusions may also involve the right ventricle and result in a preload dependent condition.(23-25) While limited by sample size, our results suggests that specifically avoiding NTG use in inferior STEMI, which is common in EMS systems, may be misguided. One quarter of the local EMS agencies in the state of California, for example, currently prohibit the use of NTG in inferior STEMI.(26) This analysis would benefit from additional study with a larger sample size and specific information about the infarct territory. Further studies are needed to determine which patients, in particular, are at increased risk for hypotension when treated with NTG.[1]Perhaps NTG is also safe for treating patients with inferior ischemia and even right ventricular ischemia. Footnotes: [1] Safety and Effectiveness of Field Nitroglycerin in Patients with Suspected ST Elevation Myocardial Infarction. Bosson N, Isakson B, Morgan JA, Kaji AH, Uner A, Hurley K, Henry TD, Niemann JT. Prehosp Emerg Care. 2018 Dec 17:1-9. doi: 10.1080/10903127.2018.1558318. [Epub ahead of print] PMID: 30556765 [2] Treatment Protocol: Chest Pain */ Acute MI Reference No. 1244 LA County Paramedic Protocols Los Angeles County Department of Health Services – Emergency Medical Services Protocol .















Subscribe to RogueMedic.com