The title of this meta-analysis suggests that it is important for us to have evidence in order to withhold treatments that are based on assumptions and anecdotes, rather than based on evidence. We should not even suggest this. Fortunately, the neonatal resuscitation guidelines have recommended not using the assumption-based and anecdote-based treatment since 2010.
 The authors of this summary of the meta-analysis qualify this meta-analysis with a list of the weaknesses of the research. This is important for every analysis of research, but is it relevant, when there is no good reason to recommend the traditional intervention?
The authors of this summary of the meta-analysis qualify this meta-analysis with a list of the weaknesses of the research. This is important for every analysis of research, but is it relevant, when there is no good reason to recommend the traditional intervention?
Before 2000, resuscitation guidelines recommended 100% Fio2 for newborn respiratory support.6 However, hyperoxemia caused by high Fio2 results in the formation of free radicals, which can damage the lungs, brain, eyes, and other organs.7 Hypoxemia may also lead to harm. Literature in the early 2000s suggested no harm with room air resuscitation in term neonates, but also potentially an improvement in short-term mortality.8 In accordance with this literature, in 2010 and 2015 ILCOR recommended using room air for the initial resuscitation of term neonates.9, 10 [1]
 The authors of this summary of the meta-analysis qualify this meta-analysis with a list of the weaknesses of the research. This is important for every analysis of research, but is it relevant, when there is no good reason to recommend the traditional intervention?
The authors of this summary of the meta-analysis qualify this meta-analysis with a list of the weaknesses of the research. This is important for every analysis of research, but is it relevant, when there is no good reason to recommend the traditional intervention?
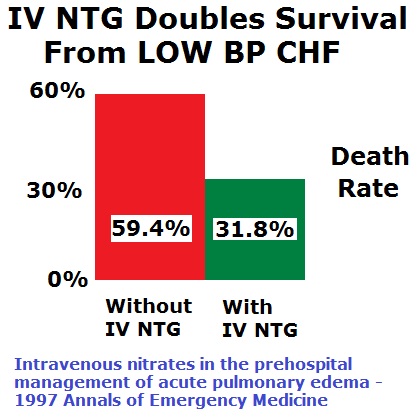
According to these results with low evidence certainty, room air reduces short-term mortality compared with 100% Fio2 among term neonates requiring respiratory support at birth. Despite the low-quality evidence, these results are consistent across studies with low heterogeneity. The effect of intermediate Fio2 levels is not known and may benefit from further study. [1]These are not reasons to reconsider, or oppose, the withholding of any treatments that are based on assumptions and anecdotes, rather than based on evidence. The burden of proof is on those promoting any intervention. In the absence of valid evidence, we should limit ourselves to interventions that are supported by high quality evidence. For epinephrine in cardiac arrest, there is no high quality evidence of benefit. The highest quality evidence is evidence of harm from epinephrine. The same is true for amiodarone, ventilation in cardiac arrest not due to a respiratory problem, furosemide in ADHF/CHF (Acute Decompensated Heart Failure/Congestive Heart Failure), and many other treatments we provide to patients, but definitely not for the benefit of patients. We need to stop putting patients last in treatment decisions. The neonatal resuscitation guidelines are correct in their rejection of supplemental oxygen for neonatal resuscitation and the guidelines should not be changed. Footnotes: [1] Does Room Air Reduce Mortality Among Term Neonates Requiring Respiratory Support at Birth? Brit Long, MD (EBEM Commentator), Michael D. April, MD, DPhil (EBEM Commentator) Department of Emergency Medicine, San Antonio Uniformed Services Health Education Consortium, Fort Sam Houston, TX Annals of Emergency Medicine October 2019, Volume 74, Issue 4, Pages 509–511 DOI:&nbps;https://doi.org/10.1016/j.annemergmed.2019.03.017 Free Full Text from Annals of Emergency Medicine. .








Subscribe to RogueMedic.com