Why treat hypoglycemia with 10% dextrose (D10), rather than the more expensive, potentially more harmful, and less available, but traditional treatment of 50% dextrose (D50)? Why not? The only benefit of 50% dextrose appears to be that it is what people are used to using, but aren’t we used to starting IVs (IntraVenous lines) and running fluids through the IVs?
We should be much more familiar with running in fluid, than in pushing boluses of syrup.
What happens when we have temporary shortages of 50% dextrose? Do we stop treating hypoglycemia? Are we supposed to panic, because we can no longer follow tradition? No. We give the more appropriate, and lower, dose of the much lower concentration of dextrose. We provide better care because of our need.
Despite the traditional use of D50, there is a minimal amount of data to support it as the standard of care.[1]
Is 10% dextrose the perfect treatment for hypoglycemia? No, but it does appear to be less likely to cause harm than the current overtreatment with 50% dextrose.
Seven patients had a drop in blood glucose after D10 administration, all of 10 mg/dL or less except for one patient with a drop of 19 mg/dL who had an insulin pump infusing that was not removed by EMS personnel during D10 infusion.[1]
Is that any different from what happens with 50% dextrose? If this is different from D50, how does the potential harm from giving too much dextrose to most hypoglycemic patients compare to the potential harm of giving a first that is too small to fewer than 1% of hypoglycemia patients?
There were no reported adverse events related to dextrose infusion. Six patients who received intravenous D10 were pronounced dead in the field during the period of study. On investigator review, all patients had altered level of arousal or were in cardiac arrest prior to arrival of EMS personnel and their deaths were deemed to be unrelated to dextrose administration.[1]
Dextrose does not reverse death, so there is no reason to expect a better outcome for dead patients with a higher concentration of a drug that does not reverse death. Go read the excellent review of the evidence on hypoglycemia, death, and the potential of dextrose to improve outcomes from death.[2]
But is 10% really better? We don’t have any good research, but is there any good reason to give all 25 grams of dextrose in a syringe of 50% dextrose if the patient wakes up before the full dose has been administered? Would we continue to give the entire syringe of morphine, or fentanyl, or most of the other drugs that we give, if our assessment shows that the patient no longer meets the protocol criteria for administration of the drug?
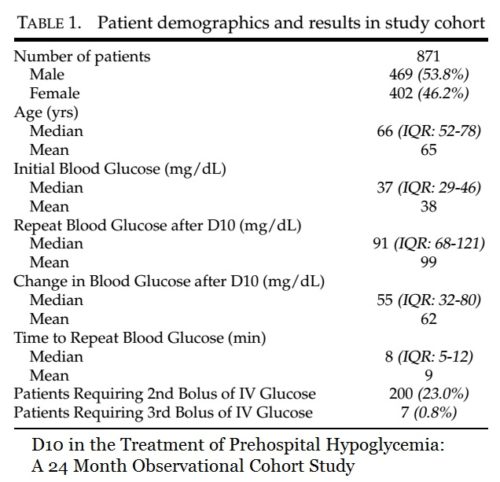
76% of patients received only 10 grams of dextrose, rather than the usual 25 grams. While it is not known if any of these patients required any further dextrose, or oral glucose, while in the hospital, they should have been awake enough to take any further dextrose orally, as they would the rest of the time.
23% of patients received only 20 grams of dextrose, rather than the usual 25 grams.
Fewer than 1% of hypoglycemia patients received a dose as large as we traditionally give.
We do not appear to be concerned with harm from administering more aggressive treatment than is justified by the evidence.
We do appear to be concerned about our anxiety of deviating from the traditional too much is not enough approach to hypoglycemia.
–
Footnotes:
–
[1] D10 in the Treatment of Prehospital Hypoglycemia: A 24 Month Observational Cohort Study.
Hern HG, Kiefer M, Louie D, Barger J, Alter HJ.
Prehosp Emerg Care. 2017 Jan-Feb;21(1):63-67. doi: 10.1080/10903127.2016.1189637. Epub 2016 Dec 5.
PMID: 27918858
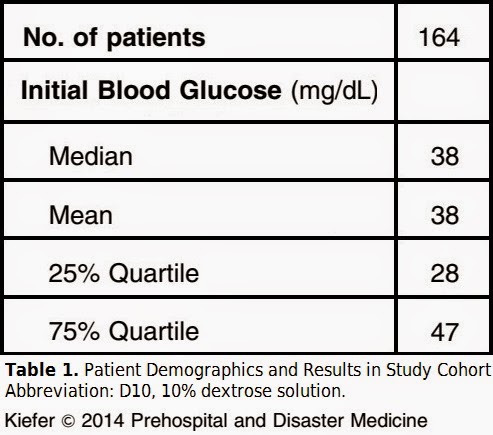
Of the 1,323 patients administered D10 during the study period, the 452 patients excluded from the study cohort for the aforementioned reasons were similar demographically to the study cohort. The median initial blood glucose was the same at 37 mg/dL and the median age was also 66. There were slightly more women at 229 (51%) in the excluded group compared to the cohort.
–
[2] Using Dextrose in Cardiac Arrest
Wednesday, March 14, 2012
Mill Hill Ave Command
Dr. Brooks Walsh
Article
–
Hern, H., Kiefer, M., Louie, D., Barger, J., & Alter, H. (2016). D10 in the Treatment of Prehospital Hypoglycemia: A 24 Month Observational Cohort Study Prehospital Emergency Care, 21 (1), 63-67 DOI: 10.1080/10903127.2016.1189637
.








.jpg)




Subscribe to RogueMedic.com