–
Continuing from Part I.
The authors do not find dramatic differences between fentanyl and morphine in their ability to relieve pain in patients who are not hypotensive. In the discussion, they begin to give their reasons for not wanting to use fentanyl.
Why?
I don’t know why they are not fond of fentanyl, but this is what they write in their discussion.
Our study opens the door for debate regarding the value of including fentanyl in limited formularies such as medical helicopters and ambulances given its higher cost and lack of any detectable advantages when compared to morphine. Whereas at our institution fentanyl costs approximately the same as morphine, costs may vary widely in other institutions.[1]
The authors state that their cost is about the same for morphine and for fentanyl, but they think that the possibility that someone somewhere might be paying a lot more for fentanyl is reason enough to limit their choices to morphine.
Both drugs are available as generics, so there does not appear to be any reason to bring a hypothetical difference in price into the discussion. Both generic drugs are affected by the current drug shortages.
If we are much more concerned about giving morphine to hypotensive patients, than we are about giving fentanyl to hypotensive patients, is that worth a bit of a premium in the price of fentanyl?
I think so. More on fentanyl and hypotensive patients in a little bit.
There is also the question of whether including fentanyl in prehospital formularies is worth the risk given its abuse potential among medical staff. Although surveillance data suggest that nationally, fentanyl is one of the least abused drugs in the non-physician population, fentanyl abuse by physicians is a well-recognized concern (24,25).[1]
The first reference does not even mention fentanyl abuse. the second reference appears to be there as a reference for the lack of abuse by non-physicians.
There is no reference for the statement that fentanyl abuse by physicians is a well-recognized concern.
Is fentanyl more of a concern than morphine?
Is fentanyl less of a concern than morphine?
There is nothing in this paper to answer that question. Are the authors using a traditional doctors’ tale an old wives’ tale?
It looks that way.
–
There was no detectable difference with the limited number of patients, the limited dosing of medication, and the refusal to include patients with a blood pressure that was not at least 10 points above where hypotension begins.
Patients were excluded if they reported an allergy to morphine or fentanyl, or if they were hypotensive before receiving the first dose of the study drug (systolic blood pressure < 100 mm Hg).[1]
It isn’t as if they would have been giving large doses.
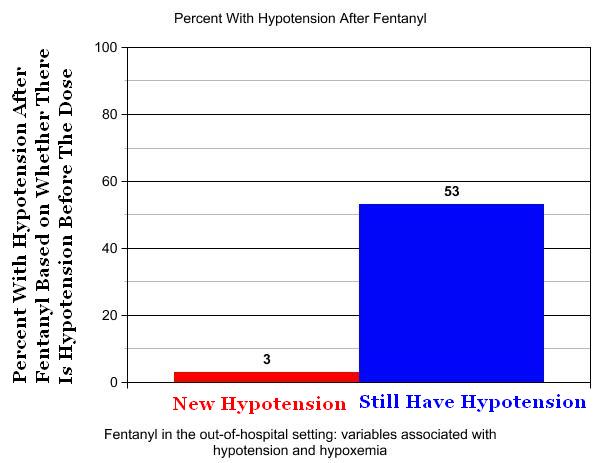
It isn’t as if there is a significant concern that fentanyl will cause hypotension.
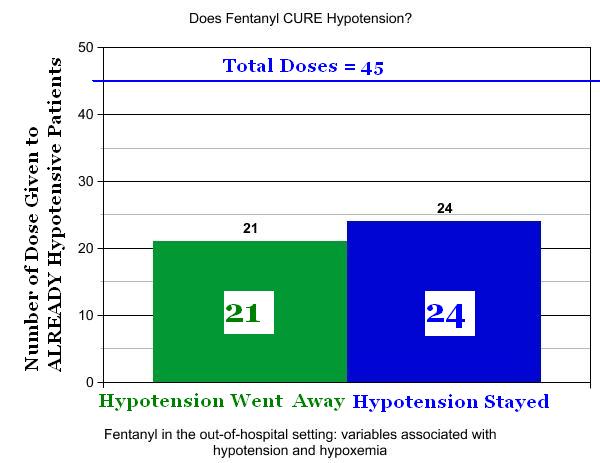
Fentanyl appears to be one of our most effective treatments for getting rid of hypotension.
There was a 47% chance that a hypotensive patient would no longer be hypotensive after a dose of fentanyl.
–
the safety of fentanyl as demonstrated in the current study may be related to more conservative dosing in unstable patients, but the parallel message is that experienced EMS crews are able to exercise judgment in determining which patients should receive cautious drug dosing.[2]
Should we assume that there is no judgment going into the dosing of patients?
experienced EMS crews are able to exercise judgment in determining which patients should receive cautious drug dosing.
–
When should we expect hypotension after giving a dose of fentanyl?
When the patient is already hypotensive.
I have written more about this study.[3]
The study is not a bad idea, since the information on the lack of hypotensive effect of fentanyl[2] was not yet published. However, the conclusions are not justified by the results of this study.
The conclusions may best be described as imaginative.
The authors seem to be experiencing a case of the vapors and might want to consider taking some anti-anxiety medication.
According to the available research, which is much more extensive than this study, fentanyl is very safe, even when the patient is hypotensive.
There is less evidence to demonstrate that the morphine is safe for treating hypotensive patients with pain, but that does not appear to be a concern of the authors, even though the pain of hypotensive patients should be the concern of all of us who treat hypotensive patients.
Is fentanyl expensive?
No.
Is fentanyl effective?
Yes.
Is fentanyl dangerous?
Fentanyl is one of the safest drugs we use.
The ignorance of those on the pushing end of the fentanyl syringe is what is dangerous.
The problem is not the fentanyl, but the ignorance.
–
Footnotes:
–
[1] The Effectiveness and Adverse Events of Morphine versus Fentanyl on a Physician-staffed Helicopter.
Smith MD, Wang Y, Cudnik M, Smith DA, Pakiela J, Emerman CL.
J Emerg Med. 2012 Jul;43(1):69-75.
PMID: 21689900 [PubMed – in process]
There is one unusual aspect to the study that does not appear to affect the outcome, but raises questions about how many obstacles to research we create, when the obstacles may not be valid.
The study was fully reviewed by our Institutional Review Board, and given that both treatment arms are considered acceptable practice with equal risk, informed consent was not deemed necessary for this study. Upon completion of participation, each patient was given a verbal and written debriefing of his or her study involvement.[1]
–
[2] Fentanyl in the out-of-hospital setting: variables associated with hypotension and hypoxemia.
Krauss WC, Shah S, Shah S, Thomas SH.
J Emerg Med. 2011 Feb;40(2):182-7. Epub 2009 Mar 27.
PMID: 19327928 [PubMed – in process]
Full Text PDF Download at medicalscg.
–
[3] Fentanyl in the out-of-hospital setting: variables associated with hypotension and hypoxemia
Rogue Medic
Fri, 27 May 2011
Article
Chart Version – Fentanyl in the out-of-hospital setting: variables associated with hypotension and hypoxemia
Rogue Medic
Sun, 05 Jun 2011
Article
Safety of prehospital intravenous fentanyl for adult trauma patients
Rogue Medic
Thu, 03 May 2012
Article
–
Smith MD, Wang Y, Cudnik M, Smith DA, Pakiela J, & Emerman CL (2012). The Effectiveness and Adverse Events of Morphine versus Fentanyl on a Physician-staffed Helicopter. The Journal of emergency medicine, 43 (1), 69-75 PMID: 21689900
–
Krauss WC, Shah S, Shah S, & Thomas SH (2011). Fentanyl in the out-of-hospital setting: variables associated with hypotension and hypoxemia. The Journal of emergency medicine, 40 (2), 182-7 PMID: 19327928
.













{kind=link}
Subscribe to RogueMedic.com