There is a study of the frequency of intubation among emergency physicians in the current Annals of Emergency Medicine. This study is accompanied by a discussion, which unfortunately does not question the assumption that intubation improves outcome. There is very little evidence to suggest that intubation improves outcomes. That evidence is only using paramedics with the highest success rates – much higher than your average paramedic.

Image credit. The unquestioned assumption is that excellent intubation performance improves outcomes, rather than that excellent intubation performance causes less harm than average intubation performance, or below average performance. We do not have any good evidence to support the wishful thinking that paramedics, or even much more experienced emergency physicians, improve outcomes by intubating patients. We just assume this, because we don’t really want to know. If we decide to be honest and actually find out the effect of intubation, how will we handle it if the results show that we are harming more patients than we are helping? The Cardiac Arrhythmia Suppression Trial was only started because the proponents of the different antiarrhythmics (encainide, flecainide, and moricizine) wanted to prove that their drug was better than all of the rest. They even agreed to include a placebo arm, although the doctors did not like the idea of depriving patients of such beneficial treatment.
Kerrey BT, Wang H.
Ann Emerg Med. 2019 Dec;74(6):795-796. doi: 10.1016/j.annemergmed.2019.06.022. Epub 2019 Aug 19. No abstract available.
PMID: 31439364
The article above is commentary on the article below:
Procedural Experience With Intubation: Results From a National Emergency Medicine Group.
Carlson JN, Zocchi M, Marsh K, McCoy C, Pines JM, Christensen A, Kornas R, Venkat A.
Ann Emerg Med. 2019 Dec;74(6):786-794. doi: 10.1016/j.annemergmed.2019.04.025. Epub 2019 Jun 24.
PMID: 31248674
[2] Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial.
Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL, et al.
N Engl J Med. 1991 Mar 21;324(12):781-8.
PMID: 1900101
Free Full Text from N Engl J Med.
[3] Blood-Letting
Br Med J.
1871 March 18; 1(533): 283–291.
PMCID: PMC2260507
Greater intubation experience in paramedics is associated with improved patient outcomes2; does a similar relationship exist for emergency physicians?[1]

Image credit. The unquestioned assumption is that excellent intubation performance improves outcomes, rather than that excellent intubation performance causes less harm than average intubation performance, or below average performance. We do not have any good evidence to support the wishful thinking that paramedics, or even much more experienced emergency physicians, improve outcomes by intubating patients. We just assume this, because we don’t really want to know. If we decide to be honest and actually find out the effect of intubation, how will we handle it if the results show that we are harming more patients than we are helping? The Cardiac Arrhythmia Suppression Trial was only started because the proponents of the different antiarrhythmics (encainide, flecainide, and moricizine) wanted to prove that their drug was better than all of the rest. They even agreed to include a placebo arm, although the doctors did not like the idea of depriving patients of such beneficial treatment.
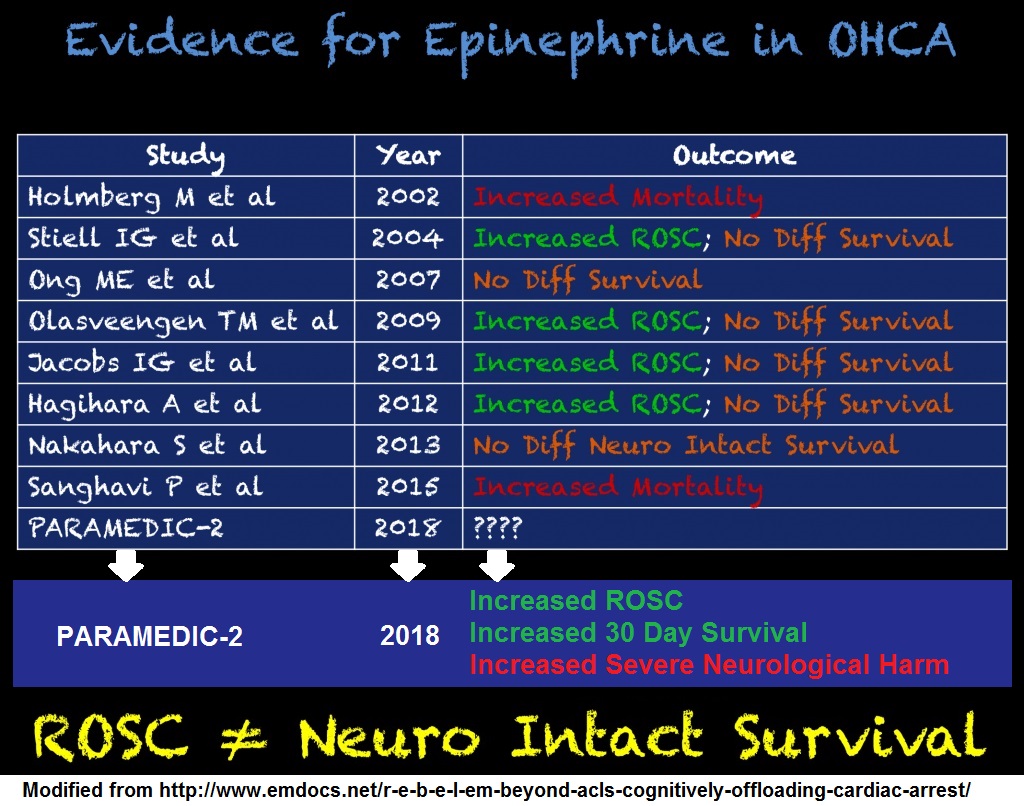
CONCLUSIONS: There was an excess of deaths due to arrhythmia and deaths due to shock after acute recurrent myocardial infarction in patients treated with encainide or flecainide.[2]People who had frequent ectopic heart beats – PVCs (Premature Ventricular Contractions) after a heart attack were more likely to die than people who did not have frequent PVCs. The obvious solution – the equivalent of intubation and blood-letting – was to give drugs that will get rid of the PVCs. The problem is that the PVCs were not the problem. The PVCs were just a sign of the problem. The drugs made the actual problem with the heart worse, while making the heart appear to be better. The same is true of blood-letting and may be true of intubation. Abundant evidence for the obvious benefits of blood-letting are quoted in the footnotes.[3] If intubation is harmful, do we want to know? If intubation by the average paramedic is harmful, do we want to know? If intubation by the average emergency physician is harmful, do we want to know? It isn’t as if we take intubation seriously. If we did take intubation seriously, we would practice much, much more than we do. In stead, we make excuses for failing to practice something that we claim is life-saving, because we are too arrogant to admit that practice is important to develop and maintain any skill. Practicing on even the most basic mannequin should be done before every shift, whether you are a paramedic or an emergency physician. Unless you have a 99%, or better, success rate on hundreds of patients. Footnotes: [1] Intubation by Emergency Physicians: How Often Is Enough?
Kerrey BT, Wang H.
Ann Emerg Med. 2019 Dec;74(6):795-796. doi: 10.1016/j.annemergmed.2019.06.022. Epub 2019 Aug 19. No abstract available.
PMID: 31439364
The article above is commentary on the article below:
Procedural Experience With Intubation: Results From a National Emergency Medicine Group.
Carlson JN, Zocchi M, Marsh K, McCoy C, Pines JM, Christensen A, Kornas R, Venkat A.
Ann Emerg Med. 2019 Dec;74(6):786-794. doi: 10.1016/j.annemergmed.2019.04.025. Epub 2019 Jun 24.
PMID: 31248674
[2] Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial.
Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL, et al.
N Engl J Med. 1991 Mar 21;324(12):781-8.
PMID: 1900101
Free Full Text from N Engl J Med.
[3] Blood-Letting
Br Med J.
1871 March 18; 1(533): 283–291.
PMCID: PMC2260507
Physicians observed of old, and continued to observe for many centuries, the following facts concerning blood-letting..
1. It gave relief to pain. . . . .
2. It diminished swelling. . . . .
3. It diminished local redness or congestion. . . . .
4. For a short time after bleeding, either local or general, abnormal heat was sensibly diminished.
5. After bleeding, spasms ceased, . . . .
6. If the blood could be made to run, patients were roused up suddenly from the apparent death of coma. (This was puzzling to those who regarded spasm and paralysis as opposite states; but it showed the catholic applicability of the remedy.)
7. Natural (wrongly termed ” accidental”) hacmorrhages were observed sometimes to end disease. . . . .
8. . . . venesection would cause hamorrhages to cease.







{kind=link}
Subscribe to RogueMedic.com