You watch the video and wonder how could anyone be so callous and cold, to leave someone outside with only a hospital gown to wear – especially when it is so cold outside.
Is what we are seeing callous, or uncaring?
In the video farther down, there is a nice discussion of the problems, which are much more complicated than somebody being refused care for some bad reason.
I found a site that did mention her clothes being with her, but stated with her clothes and belongings scattered on the sidewalk. Here is the picture they posted. The clothes are in plastic patient belongs bags.
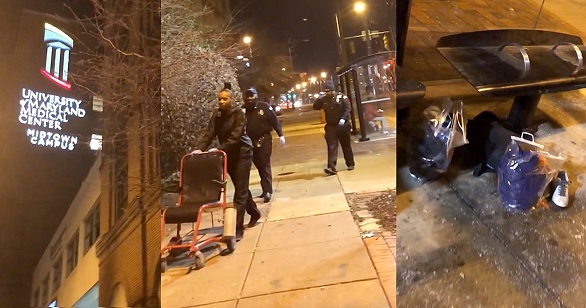
Psychotherapist Imamu Baraka was walking near the University of Maryland Medical Center’s midtown campus location when he saw a woman being dropped off by security at a bus stop with her clothes and belongings scattered on the sidewalk.[1]
Why didn’t she put her clothes on?
One of the first things discharged patients will do, if they can, is put their own clothes on.
There is no evidence that anyone was refused care. That would be an EMTALA (Emergency Medical Treatment and Labor Act) violation, resulting in a very big fine, which would be reported. Maybe I am wrong, but I do not expect that an investigation will end with any finding of any refusal to provide care.
But we saw it on the video!
No. I think that you saw someone being removed from private property for bad behavior in a hospital gown, and she refused to put on her own clothes on (the clothes in her bag) for reasons of her own.
Here is a video explaining this in more detail, but a couple of notes about people mentioned in the video.
Charlie Gard was an infant with irreversible MDDS (Mitochondrial DNA Depletion Syndrome). The doctors and nurses seem to have understood this, but parents, politicians, preachers, and the press thought that it would be a good idea to torture Charlie Gard with an experimental treatment with no expectation of a better outcome.
How would Solomon decide? To torture, on the ridiculously small chance of a better outcome, or to do not further harm?
Peter Gallogly is a doctor, who was selectively recorded on video to make it seem as if his unprofessional behavior was unprovoked. If you watch the video of Dr. Gallogly, realize that it is edited to distort reality. If you watch the ironically named Project Veritas videos of abortion clinics, they are similarly edited to distort reality, which is why they have been rejected as evidence in court. You might as well watch a Michael Moore film, if you want a highly edited distortion of reality.
The Delnor nurse protected staff from an escaped prisoner, when the corrections officer apparently fled. The nurse ended up being abducted for hours, grazed by a bullet, pistol whipped, and raped, but was reported as being unharmed after the inmate was killed.
We need to learn how to find out accurate information for ourselves, rather than blindly accept propaganda from far left or far right news sources. Even the mainstream news will often get information in specialized fields wrong and not realize it. When the story is from a specialized field, such as medicine, we should obtain our information from trustworthy people in that field.
More information on Charlie Gard.
More information on Peter Gallogly.
More information on the Delnor nurse.
All of the videos are from ZDoggMD.com
–
Footnotes:
–
[1] Video shows Baltimore hospital discharging half-naked woman into cold winter night
Ana Valens
Jan 11 at 7:27AM | Last updated Jan 12 at 3:36AM
The Daily Dot
Article
.






Subscribe to RogueMedic.com