–
One of the myths of treatment for CHF/ADHF (Congestive Heart Failure/Acute Decompensated Heart Failure) is that the patients are fluid overloaded. We MUST make the patient pee.
If you want to live, you have to pee!

Pee or die!
This has been studied. all the way back in 1978 –

The normal patients had 22% more total plasma volume.
The normal patients had 21% more total blood volume.
The need to remove fluids is based on what?
It is interesting that this study was of patients treated with oxygen, morphine, and furosemide. Only oxygen is still important in the acute treatment of CHF/ADHF.
There were no significant differences in the parameters measured or calculated between nine patients with prior history of acute pulmonary edema and the 12 patients in whom pulmonary edema occurred for the first time. There were also no significant differences in these parameters between the 11 patients who had been previously treated with diuretics and the remaining ten patients.[1]
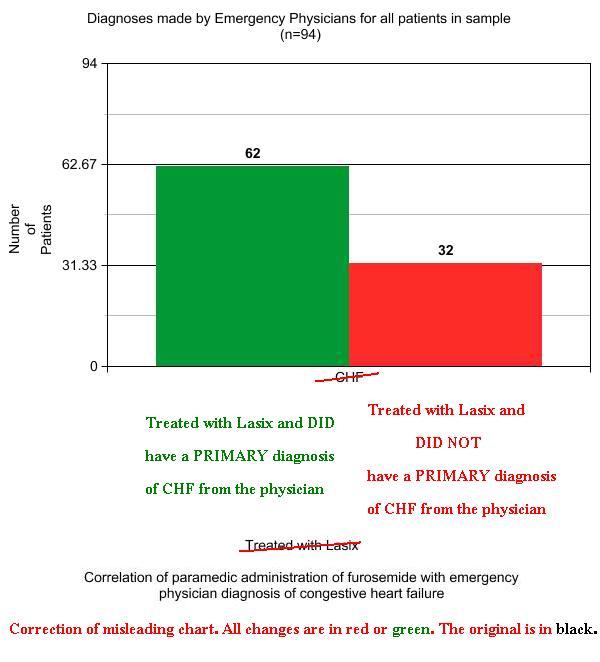
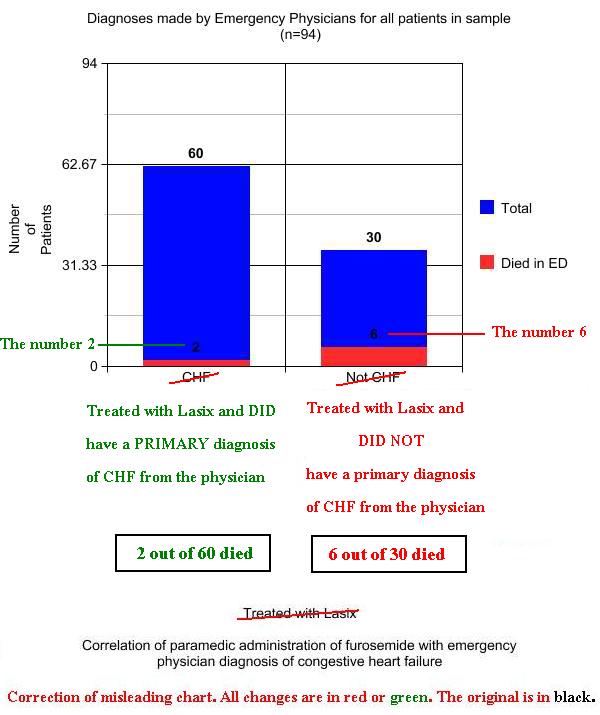
We give have been trained to give furosemide (Lasix – frusemide in Commonwealth countries) because CHF = Too much fluid.
How long do we need to hold on to our myths?
How long can we perpetuate dangerous traditions?
Afterward, these patients need to receive fluid, because we have made them even more dehydrated – for no benefit.
–
Correction – These appear to be ICU (Intensive Care Unit) patients. I had mistakenly assumed these were ED (Emergency Department) patients. This also weakens the conclusions I was drawing from the study. I had been misreading the Center for the Critically Ill as a fancy name for the ED (A&E in Commonwealth countries).
Read Doesn’t that study prove Lasix works? for a more in depth explanation.
Footnotes:
–
[1] Blood volume prior to and following treatment of acute cardiogenic pulmonary edema.
Figueras J, Weil MH.
Circulation. 1978 Feb;57(2):349-55.
PMID: 618625 [PubMed – indexed for MEDLINE]
Free Full Text Download from Circulation in PDF format
–
Figueras J, & Weil MH (1978). Blood volume prior to and following treatment of acute cardiogenic pulmonary edema. Circulation, 57 (2), 349-55 PMID: 618625
–
Edited 12-27-2018 to add the necessary paragraph explaining that this is not an ED study and the link to where I provide more detail.
.









.jpg)





Subscribe to RogueMedic.com