Does 1 + 1 always equal 3?
No.
If you do not give all of the medication in a syringe, vial, ampule, you are rounding off. This is where significant figures matter.[1]
1+1 does equal 3 for sufficiently high values of 1.
For those who do not understand this –
Consider a morphine syringe with a volume of 1 ml that contains a total dose of 10 mg.
We intend to give 1 mg.
Can we give exactly 1 mg?
I cannot.
We give an approximation of 1 mg.
What is considered to be 1 mg?

0.50001 mg should be rounded to 1 mg if we are not using decimal places. We probably do not have the precision to measure that accurately. If we did, we should use all of the significant digits in our documentation.
I am using this as an example to point out that with no decimal places 0.50001 mg is 1 mg.
We round off to the nearest significant digit.
If we are not using decimals, then 1.49999 mg is also 1 mg.
We will not be measuring that as carefully, either.
What we will be doing is trying to get close to 1 mg, but that could be 1.4 mg, or 1.3 mg, or 1.2 mg, or 1.1 mg, 0.9 mg, or 0.8 mg, or 0.7 mg, or 0.6 mg, or 0.5 mg.
How precisely can we measure the amount?
If we tend to underestimate the doses we are giving, we could be giving a couple of doses of 1.3 mg.
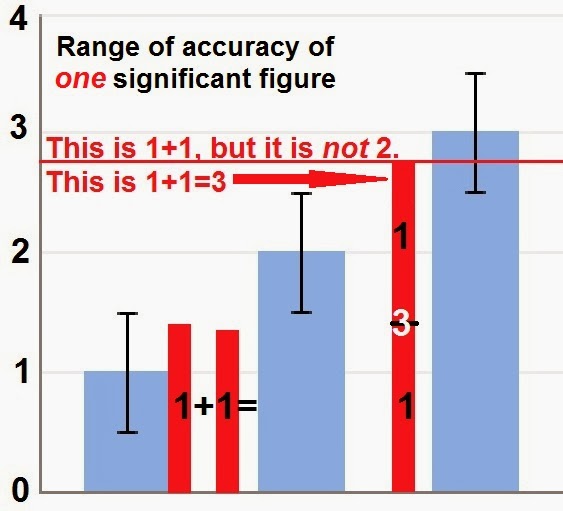
1.3 + 1.3 = 2.6, which is rounded to 3.
1 + 1 = 3.
If I gave 1.3 mg and 1.3 mg to the same patient, I gave 1 mg + 1 mg and the
1.4 can be rounded off to 1.
If there are no significant digits beyond the 1, then the value of 1 is anywhere from 0.6 to 1.4.
Add a couple of 1s that add up to 2.5, or greater, and you have 3.
1.2 + 1.3 = 2.5, which is rounded to 3.
When rounded to one significant digit, 1.2 = 1, 1.3 = 1, 1.4 = 1, and 2.5 = 3.
That is not what we generally think of when we think of 1 + 1 = 3.
We assume a precision that may not be there.
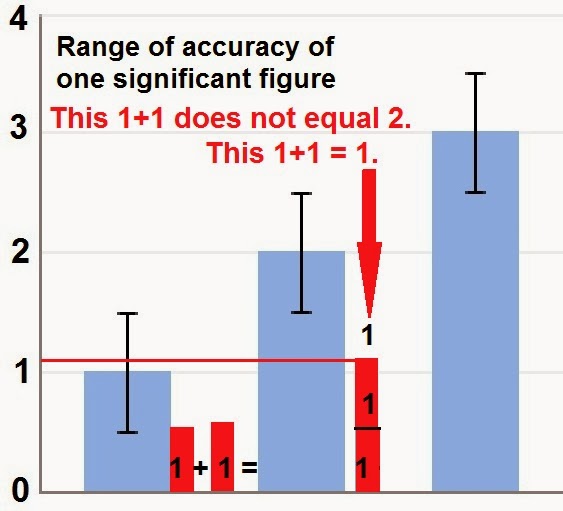
Error bars do not always result in excess.
We can end up with a small number due to wide error bars.
1+1 can equal 1 for sufficiently low values of 1.
So,
how
accurate
are
we?
–
Footnotes:
–
[1] Significant figures
Wikipedia
Article
.










Subscribe to RogueMedic.com