Last night I called in to the EMS Roundtable because the topic was one of the most important in EMS – critical thinking.[1]
Critical thinking is the intellectually disciplined process of actively and skillfully conceptualizing, applying, analyzing, synthesizing, and/or evaluating information gathered from, or generated by, observation, experience, reflection, reasoning, or communication, as a guide to belief and action.[2]
More simply, in EMS critical thinking is how we make good decisions based on the limited information available in the emergency setting.
In EMS we definitely can be too safe.
Not applying a tourniquet, because What if the tourniquet causes a problem?
That is being too safe.
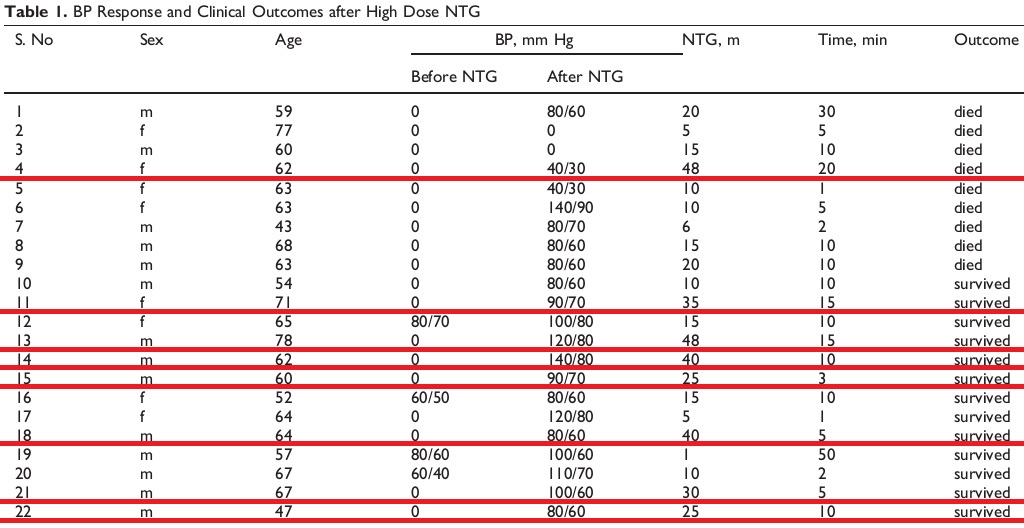
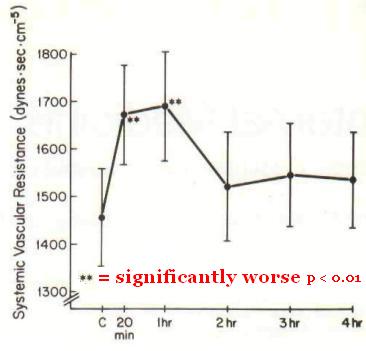
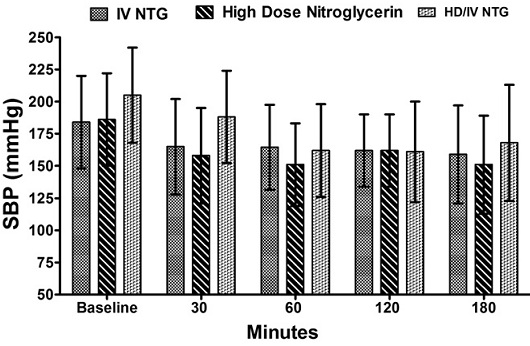
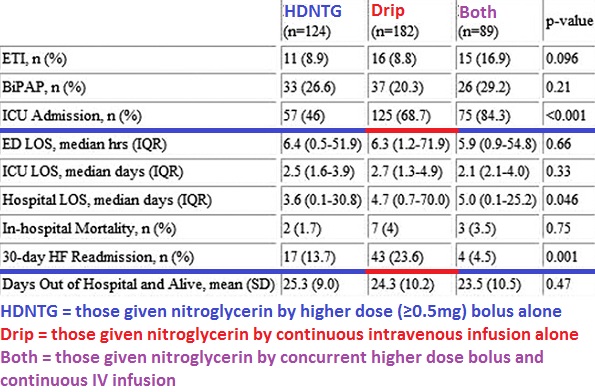
Not giving large doses of NTG to a hypertensive CHF patient, because What if the NTG causes the pressure to bottom?
That is being too safe.
Strapping someone to a backboard with straps and a collar, Just to be safe.
How is that not being too safe?
Where is there any evidence that spinal immobilization is safe?
Not sedating (or not adequately sedating) an excited delirium patient, because What if he stops hyperventilating?
That is being too safe.
These are some of the things that need to be considered when we engage in critical thinking.
Show Notes:
Guest Dan Limmer: http://limmercreative.com
Live Call-in Tim Noonan: http://roguemedic.com
Chat Room:
Jim Hoffman: http://emsofficehours.com
Tom Bouthillet: http://EMS12Lead.com
–
Footnotes:
–
[1] The Art of Critical Thinking
The EMS Roundtable
Wed, April 24, 2013 07:00 pm
Podcast page.
–
[2] Defining Critical Thinking
Criticalthinking.org
Web page
.







Subscribe to RogueMedic.com