Click on the image to make it larger.
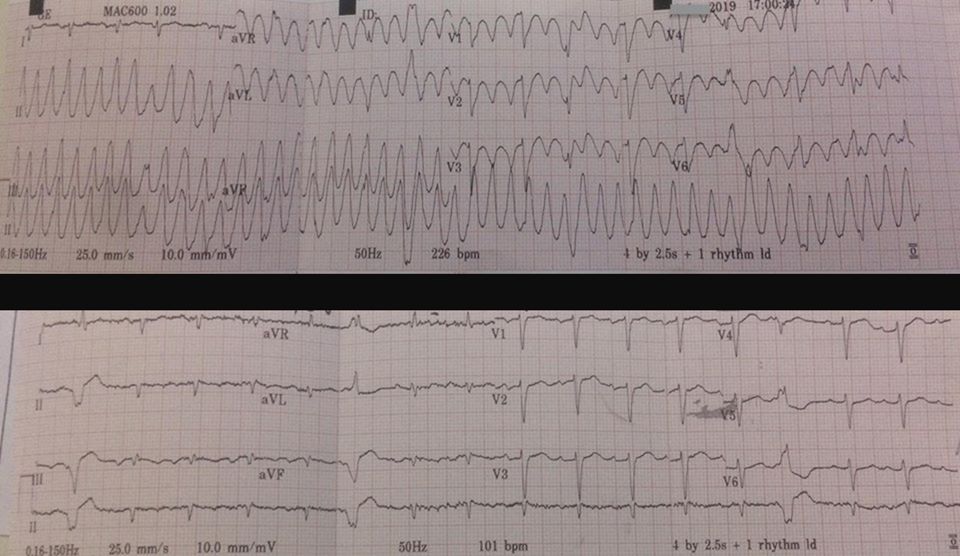
Apparently, the second 12 lead was after 150 mg of amiodarone. The hilarity is the amiodarone.
I received this in an email. It is reported to have been posted on Facebook, but I choose not to have access to Facebook, so I do not have any more details. I am occasionally tempted to set up an account again, but I generally prefer intentional comedy.
Everything you need to know is in the first 12 lead.
Things that do not matter:
Distance to the hospital.
Time of onset.
Last meal.
National Registry certification.
Et cetera.
.






Subscribe to RogueMedic.com