
All rest and no work makes Jack a cold boy.
All rest and no work makes Jack a cold boy.
All rest and no work makes Jack a cold boy.
All rest and no work makes Jack a cold boy.
All rest and no work makes Jack a cold boy.
All rest and no work makes Jack a cold boy.
All rest and no work makes Jack a cold boy.
😎
–
The 22-year-old South Korean man is in a critical condition with hypothermia, and was put into an induced coma, after being found at Falls Creek in the state’s northeast about 4.30am.[1]
It is unusual for someone to be found at 04:30, but this guy was. Given his temperature, if he had been found at 05:00, he probably would have been pulseless and he probably would not been resuscitated.
–
Senior intensive care paramedic Patrick Gleeson said the man’s core temperature was only 24C – compared to 37C normally.
“That’s one of the coldest patients that I’ve been to in 30 years of ambulance service,” the Ambulance Victoria clinical support officer said.[1]
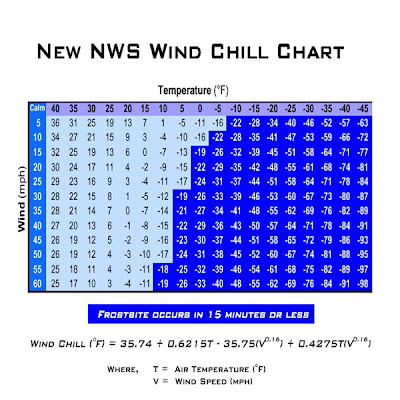
24 °C is equal to 75.2 °F. Comfortable as an air temperature. Cool as a water temperature. Very, very cold for a human body.
While this does not appear to be the time of year to consider this, it is in Australia. The difference between hypothermia in the Summer and hypothermia in the Winter is the rate of cooling.
–
Unintentional or accidental hypothermia is a serious and preventable health problem. Severe hypothermia (body temperature <30°C [86°F]) is associated with marked depression of critical body functions, which may make the victim appear clinically dead during the initial assessment. Therefore, lifesaving procedures should be initiated unless the victim is obviously dead (eg, rigor mortis, decomposition, hemisection, decapitation).[2]
–
These patients need aggressive rewarming and they need to be prevented from getting cold again.
For patients with severe hypothermia (<30°C [86°F]) with a perfusing rhythm, core rewarming is often used, although some have reported successful rewarming with active external warming techniques.408,409 Active external warming techniques include forced air or other efficient surface-warming devices.[2]
–
“It’s typically not seen in Australia.
“The only time that these sort of temperatures are recorded in patients that have survived are perhaps in Europe and Canada and the United States.”[1]
Because the temperature does not get low enough to drop a person’s body temperature down to 75 degrees quickly? Why not?
I think that it is rare anywhere. Few of us have treated patients with body temperatures this cold, but still alive. It is important to recognize the problem quickly. Remove wet clothing and dry the patient also quickly.
–
ACLS management of cardiac arrest due to hypothermia focuses on aggressive active core rewarming techniques as the primary therapeutic modality. Conventional wisdom indicates that the hypothermic heart may be unresponsive to cardiovascular drugs, pacemaker stimulation, and defibrillation; however, the data to support this are essentially theoretical.429[2]
In other words, rewarming works. Beyond rewarming, we are guessing. Since the drugs do not appear to improve survival to discharge in normothermic cardiac arrest, there is no reason to expect them to suddenly improve outcomes just because the patient is cold.
–
See also – Potentially Reversible Causes – Hypothermia.
–
Footnotes:
–
[1] Naked freezing man found alive in the snow was coldest survivor ever seen by paramedic
by Matthew Schulz and Amelia Harris
From: AAP, Herald Sun
August 11, 2011 1:18PM
Article
There are also 2 audio segments at the bottom of the page. An interview with one of the doctors and an interview with the paramedic.
–
[2] Part 12.9: Cardiac Arrest in Accidental Hypothermia
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science
Part 12: Cardiac Arrest in Special Situations
Free Full Text from Circulation with links to Free Full Text PDF Download
.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subscribe to RogueMedic.com