There have been two studies comparing epinephrine with placebo to treat out of hospital cardiac arrest. The Jacobs study was stopped early, because of interference by those who do not want to know if their medicine actually works.[1] The purpose of research is to determine, as objectively as possible, if a treatment is better than placebo nothing.
 Click on the image to make it larger.
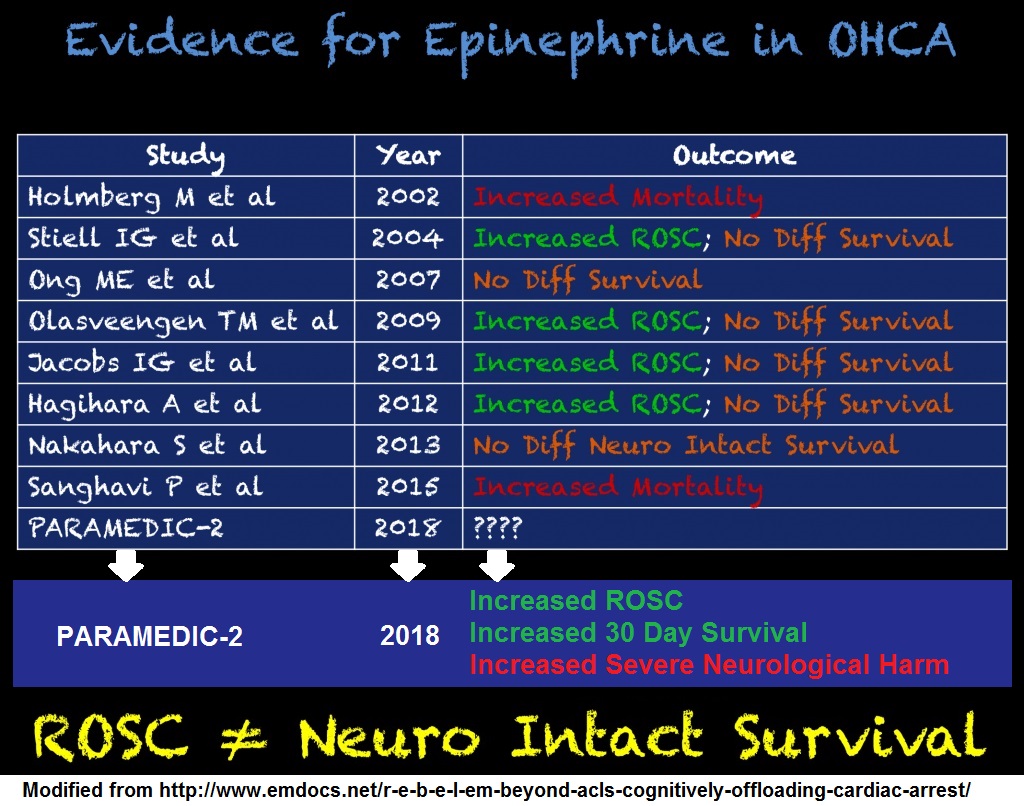
Even the small sample size shows a impressive p values of <0.001 for both ROSC (Return Of Spontaneous Circulation) and being admitted to the hospital. Unfortunately, that does not lead to outcomes that are better than placebo.
The Perkins study (PARAMEDIC2) did not find a significant difference between adrenaline (epinephrine in non-Commonwealth countries) and placebo.[2] The Jacobs study also did not find a difference, but the numbers were small, due to the interference by the less than knowledgeable. Following the Jacobs study, some intervention proponents have suggested that the problem is not a lack of evidence of benefit, but need to look at the evidence from the right perspective. The inadequate evidence is not “inadequate”, but really just misunderstood. All we need to do is use a method of analysis that compensates for the tiny sample size. A Bayesian approach will produce the positive outcome that is not justified by so few patients.[3]
What happens when the numbers are combined, so that the sample size is large enough to eliminate the need for statistical chicanery to come up with something positive?
The outcomes do not improve.
Click on the image to make it larger.
Even the small sample size shows a impressive p values of <0.001 for both ROSC (Return Of Spontaneous Circulation) and being admitted to the hospital. Unfortunately, that does not lead to outcomes that are better than placebo.
The Perkins study (PARAMEDIC2) did not find a significant difference between adrenaline (epinephrine in non-Commonwealth countries) and placebo.[2] The Jacobs study also did not find a difference, but the numbers were small, due to the interference by the less than knowledgeable. Following the Jacobs study, some intervention proponents have suggested that the problem is not a lack of evidence of benefit, but need to look at the evidence from the right perspective. The inadequate evidence is not “inadequate”, but really just misunderstood. All we need to do is use a method of analysis that compensates for the tiny sample size. A Bayesian approach will produce the positive outcome that is not justified by so few patients.[3]
What happens when the numbers are combined, so that the sample size is large enough to eliminate the need for statistical chicanery to come up with something positive?
The outcomes do not improve.
 Click on the image to make it larger.
Even the small sample size shows a impressive p values of <0.001 for both ROSC (Return Of Spontaneous Circulation) and being admitted to the hospital. Unfortunately, that does not lead to outcomes that are better than placebo.
The Perkins study (PARAMEDIC2) did not find a significant difference between adrenaline (epinephrine in non-Commonwealth countries) and placebo.[2] The Jacobs study also did not find a difference, but the numbers were small, due to the interference by the less than knowledgeable. Following the Jacobs study, some intervention proponents have suggested that the problem is not a lack of evidence of benefit, but need to look at the evidence from the right perspective. The inadequate evidence is not “inadequate”, but really just misunderstood. All we need to do is use a method of analysis that compensates for the tiny sample size. A Bayesian approach will produce the positive outcome that is not justified by so few patients.[3]
What happens when the numbers are combined, so that the sample size is large enough to eliminate the need for statistical chicanery to come up with something positive?
The outcomes do not improve.
Click on the image to make it larger.
Even the small sample size shows a impressive p values of <0.001 for both ROSC (Return Of Spontaneous Circulation) and being admitted to the hospital. Unfortunately, that does not lead to outcomes that are better than placebo.
The Perkins study (PARAMEDIC2) did not find a significant difference between adrenaline (epinephrine in non-Commonwealth countries) and placebo.[2] The Jacobs study also did not find a difference, but the numbers were small, due to the interference by the less than knowledgeable. Following the Jacobs study, some intervention proponents have suggested that the problem is not a lack of evidence of benefit, but need to look at the evidence from the right perspective. The inadequate evidence is not “inadequate”, but really just misunderstood. All we need to do is use a method of analysis that compensates for the tiny sample size. A Bayesian approach will produce the positive outcome that is not justified by so few patients.[3]
What happens when the numbers are combined, so that the sample size is large enough to eliminate the need for statistical chicanery to come up with something positive?
The outcomes do not improve.
Neither standard dose adrenaline, high-dose adrenaline,vasopressin nor a combination of adrenaline and vasopressin improved survival with a favourable neurological outcome.[4]If the Bayesian approach were appropriate, then the much larger sample size would have provided more than enough patients to confirm the optimism of the epinephrine advocates. The result is still not statistically significant. Maybe a much, much larger study will show a statistically significant, but tiny, improvement in outcomes with epinephrine, but don’t hold your breath for that. It took half a century to produce the first study, then seven more years for the second. With the cost of research and the problems coordinating such a large study, it is more likely that the guidelines will continue to recommend spending a lot of time and money giving a drug that diverts attention from the interventions that do improve outcomes. There is still no evidence that adrenaline provides better outcomes than placebo in human cardiac arrest patients. – Footnotes: – [1] Effect of adrenaline on survival in out-of-hospital cardiac arrest: A randomised double-blind placebo-controlled trial Jacobs IG, Finn JC, Jelinek GA, Oxer HF, Thompson PL. Resuscitation. 2011 Sep;82(9):1138-43. doi: 10.1016/j.resuscitation.2011.06.029. Epub 2011 Jul 2. PMID: 21745533 Free Full Text PDF Download from semanticscholar.org
This study was designed as a multicentre trial involving five ambulance services in Australia and New Zealand and was accordingly powered to detect clinically important treatment effects. Despite having obtained approvals for the study from Institutional Ethics Committees, Crown Law and Guardianship Boards, the concerns of being involved in a trial in which the unproven “standard of care” was being withheld prevented four of the five ambulance services from participating.
In addition adverse press reports questioning the ethics of conducting this trial, which subsequently led to the involvement of politicians, further heightened these concerns. Despite the clearly demonstrated existence of clinical equipoise for adrenaline in cardiac arrest it remained impossible to change the decision not to participate.– [2] A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. Perkins GD, Ji C, Deakin CD, Quinn T, Nolan JP, Scomparin C, Regan S, Long J, Slowther A, Pocock H, Black JJM, Moore F, Fothergill RT, Rees N, O’Shea L, Docherty M, Gunson I, Han K, Charlton K, Finn J, Petrou S, Stallard N, Gates S, Lall R; PARAMEDIC2 Collaborators. N Engl J Med. 2018 Aug 23;379(8):711-721. doi: 10.1056/NEJMoa1806842. Epub 2018 Jul 18. PMID: 30021076 Free Full Text from N Engl J Med. – [3] Regarding “Effect of adrenaline on survival in out-of-hospital cardiac arrest: A randomised double-blind placebo-controlled trial”. Youngquist ST, Niemann JT. Resuscitation. 2012 Apr;83(4):e105; author reply e107. doi: 10.1016/j.resuscitation.2011.09.035. Epub 2012 Jan 18. No abstract available. PMID: 22266068 Free Full Text from Resuscitation. – [4] Adrenaline and vasopressin for cardiac arrest. Finn J, Jacobs I, Williams TA, Gates S, Perkins GD. Cochrane Database Syst Rev. 2019 Jan 17;1:CD003179. doi: 10.1002/14651858.CD003179.pub2. PMID: 30653257 .







Subscribe to RogueMedic.com