.jpg)
–
Also posted over at
Paramedicine 101, which is now at EMS Blogs. Go check out the excellent material there.I will keep pointing out the problems with furosemide (Lasix) and the evidence against it. Let’s ignore the problems with giving furosemide to patients who actually have CHF/ADHF (Congestive Heart Failure/Acute Decompensated Heart Failure). Can medics correctly identify CHF/ADHF?
The EHS ePCR database identified paramedic reports in which furosemide was administered. As furosemide only appears in the CHF/pulmonary edema protocol, paramedic differential diagnosis of this was assumed by furosemide administration. Data abstraction from the EHS ePCR and ED chart included the EP primary diagnosis, considered the gold standard. Other data points collected included: demographic information; EHS treatment administered; treatment administered in the ED; adverse events and patient disposition.[1]
They do not describe their method of selecting the charts.
Was it completely random?
Was it sequential?
How did they select their sample?
There were three objectives of this study. The first was to determine agreement between paramedic administration of furosemide with EP diagnosis of CHF. The second was to examine differences in interventions administered by paramedics and in the ED by EP diagnosis of CHF. The third objective was to identify any adverse events that occurred during patient care.[1]
How much agreement on CHF/ADHF diagnoses?

It should be noted that seven patients without an ED diagnosis of CHF received ED furosemide and 43 patients received ED nitro with only eight of those having a primary diagnosis of ACS. This data put the accuracy of the primary ED final diagnosis as a reference standard into question, as it appears CHF may have been in the differential diagnosis for many patients not ultimately diagnosed with CHF. Secondary diagnoses were not sought out and included. Therefore, paramedic accuracy reported in this study may be falsely low, if CHF was part of the EP secondary diagnoses. It should also be noted that there were two patients with a diagnosis of “shortness of breath not yet diagnosed.” It is possible that these patients did indeed have CHF, but were not diagnosed until a later time during hospital care. This needs to be considered when determining paramedic diagnostic accuracy.[1]
OK. For some reason, the emergency physicians gave furosemide to 21% of the patients they diagnosed with something other than CHF/ADHF. That may be explained by the CHF/ADHF being a secondary diagnosis.
This is something that should have been included in the study. What was being treated and for what reason. From the way they describe their data, they had the actual ED physician chart, not just a diagnosis. This is something they should include in a follow-up study, especially with a larger sample size.
Since two of the patients had the diagnosis shortness of breath not yet diagnosed I will move them to the CHF/ADHF side of the graph. After all, most of the patients were diagnosed with CHF/ADHF.
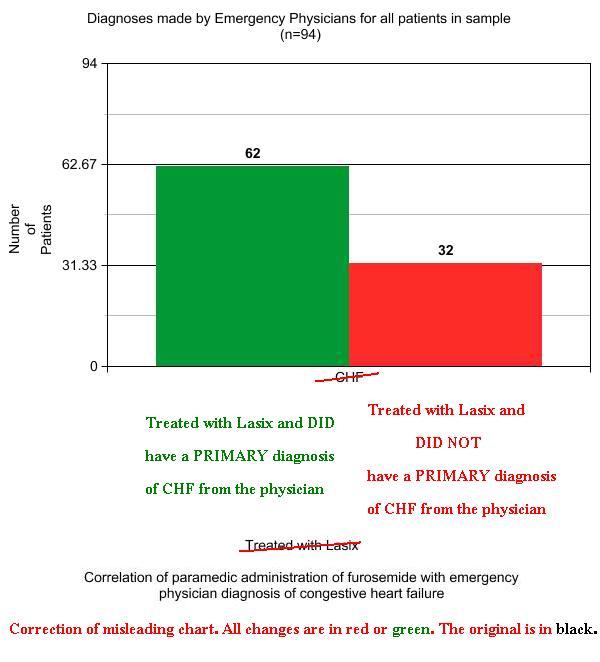
That looks so much better.
On the other hand, there are problems with the way they conclude that some patients do not have CHF/ADHF. How much higher would things be if secondary diagnoses were included?
–
It should be noted that seven patients without an ED diagnosis of CHF received ED furosemide and 43 patients received ED nitro with only eight of those having a primary diagnosis of ACS. This data put the accuracy of the primary ED final diagnosis as a reference standard into question[1]
What does NTG (NiTroGlycerin) have to do with ACS (Acute Coronary Syndrome), when examining CHF/ADHF treatment?
NTG is the most effective medication for hypertensive CHF/ADHF. Go listen to the EMCrit CHF/ADHF podcast if you doubt me. For those not hypertensive, this research certainly suggests that NTG should be studied.
NTG is not just for chest pain.
–
Data abstraction from the EHS ePCR and ED chart included the EP primary diagnosis, considered the gold standard.[1]
Maybe. Maybe not. And don’t get me started on Gold Standards.
–
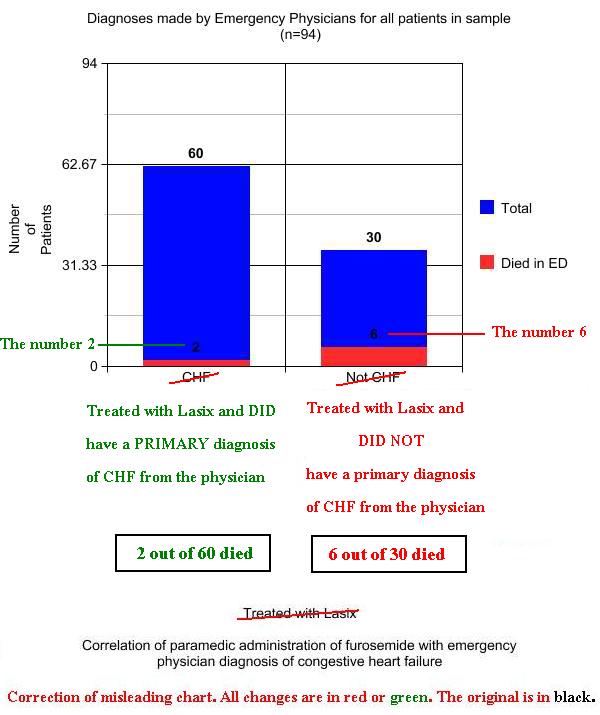
ED mortality was higher in patients with an alternate diagnosis than those diagnosed with CHF by the EP (2/60 vs. 6/34, p=0.017). As documented on ED charts, eight patients in this sample suffered adverse events other than death. These adverse events were: hypotension (n =3), heart rate problem (n =3), electrolyte imbalance (n =1), and respiratory effort decline (n = 1). All of the patients who suffered adverse events were diagnosed with CHF by the EP. Adverse events were not associated with the amount of nitroglycerin, morphine or furosemide administered.[1]
Adverse events in the ED were documented as occurring as often as death in the ED. Almost all of the deaths were in the group not diagnosed with CHF/ADHF, but all of the adverse events occurred in the group diagnosed with CHF/ADHF.
Of the six patients with an alternate diagnosis who had an outcome of death, three were diagnosed with pneumonia. Eight adverse events other than death were identified in this sample. Interestingly, all these patients were correctly identified as having CHF, which contradicts previous research which has found adverse events were more likely in patients incorrectly treated for CHF by paramedics.11,12 This indicates that furosemide should be administered with caution, even in cases where diagnosis of CHF is correct.[1]
Where is the evidence that furosemide should be administered, even if the diagnosis of CHF/ADHF is correct?
What would we want to know?
Did the patients have peripheral edema when given furosemide by EMS. Even with peripheral edema, furosemide is far from the first line drug, but without peripheral edema, it is not going to do anything good.
These patients need the best treatment possible, not the most persistent hold out from the Dark Ages.
We have known that CHF/ADHF is not primarily a fluid overload problem since the 1980s.
Why is EMS still using furosemide?
Is there any problem with a shortage of furosemide?
Not at all, but this isn’t the study to prove it.
I hope the authors use what they learned from this to design a definitive study of the prehospital use of furosemide.
–
Updated 02-07-11 to correct the uselessness of the original charts I made for this post.
More details are in Corrections of Misleading Charts.
–
Footnotes:
–
[1] Correlation of paramedic administration of furosemide with emergency physician diagnosis of congestive heart failure
Thomas Dobson, Jan Jensen, Saleema Karim, and Andrew Travers.
Journal of Emergency Primary Health Care
Vol.7, Issue 3, 2009
Free Full Text . . . . . . . Free Full Text PDF
.







Subscribe to RogueMedic.com