Yesterday, the FDA sent out a press release about the approval of Abstral brand of transdermal/transmucosal fentanyl for breakthrough pain in opioid-tolerant cancer patients.
–
The U.S. Food and Drug Administration today approved Abstral (fentanyl) transmucosal tablets to manage breakthrough pain for adults with cancer. Fentanyl immediate-release transmucosal medications are administered on the soft surfaces of the mouth (inside of the cheek, gums, tongue), or the nasal passages or throat where they dissolve and are absorbed.[1]
We know that breakthrough pain is going to happen for patients with cancer who are already taking large doses of opioids.
This progression of pain may not affect 100% of the population, but understanding the progression of cancer means that we expect that the pain will become worse as the cancer becomes worse.
Unless a patient is improving, we should expect repeated episodes of breakthrough cancer pain.
–
Abstral is indicated for the management of breakthrough pain in patients with cancer, ages 18 years and older, who already use opioid pain medication around the clock and who need and are able to safely use high doses of an additional opioid medicine. Breakthrough pain is pain that comes on suddenly for short periods of time and is not alleviated by a patient’s normal pain management plan. These patients are considered opioid tolerant because of their current opioid medication use. Only health care professionals skilled in the use of Schedule II opioids to treat pain should prescribe this drug product.[1]
Opioid-tolerant cancer patients, but only if they are at least 18 years old.
Apparently, the idea of appropriately treating breakthrough cancer pain in children is too controversial.
17 years and 11 months old = no treatment with Abstral. We must think of the children.
18 years old and it is OK to treat the patient appropriately.
This is ridiculously childish on the part of the regulators.
No. We do not need to draw the line somewhere.
We need to have competent people making patient care decisions and taking the patient’s size into consideration.
We do not need some mindless and arbitrary limit based on birthdays. That is not competent.
–
Abstral is available only through a Risk Evaluation and Mitigation Strategy (REMS) program, which is intended to minimize the risk of misuse, abuse, addiction and overdose.[1]
Most of the patients this applies to are going to die in the months after beginning use of this treatment, unless I misunderstand the proportion of patients with breakthrough pain, who will go into remission or be cured. How worried are we about the distinction between addiction and dependence at the end of life?
–
What about overdose?
Most likely, EMS calls will be for patients being cared for in the home by someone not well trained in the use of opioids, but accustomed to giving doses much larger than EMS is accustomed to giving. Another factor is that Abstral is titrated semi-aggressively using increasing doses. For this reason, the potential for dosing error is probably significantly higher than for other formulations of fentanyl. Understanding the information in the label may be beyond the abilities of many people providing care for family members at home. It is not clear how much education will be provided to the family by hospice/hospital educators.
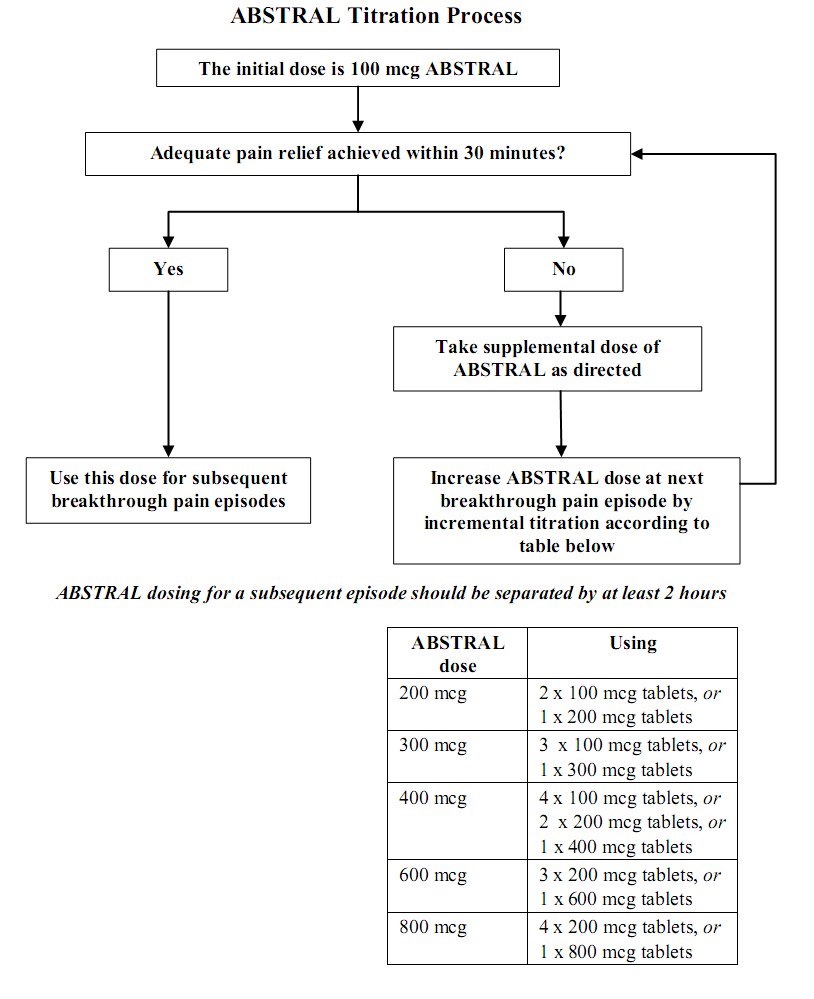
Image from FDA Label
–
1 INDICATIONS AND USAGE
ABSTRAL (fentanyl) sublingual tablets are indicated only for the management of breakthrough pain in cancer patients 18 years of age and older who are already receiving, and who are tolerant to, opioid therapy for their underlying persistent cancer pain. Patients considered opioid tolerant are those who are taking around-the-clock medicine consisting of at least 60 mg of oral morphine daily, or at least 25 mcg of transdermal fentanyl/hour, or at least 30 mg of oral oxycodone daily, or at least 8 mg of oral hydromorphone daily or at least 25 mg oral oxymorphone daily, or an equianalgesic dose of another opioid medication daily for a week or longer.ABSTRAL is contraindicated for patients who are not already tolerant to opioids because life-threatening respiratory depression and death could result at any dose in patients not on a chronic regimen of opioids. For this reason, ABSTRAL is contraindicated in the management of acute or postoperative pain, including headache/migraine, dental pain, or use in the emergency room.[2]
It is good that something is being done to address the much higher doses of opioids required by those who are opioid-tolerant. It is good that there is a realization that these doses are in an entirely different category from postoperative, migraine, and dental pain.
I do not agree that Abstral is inappropriate for the emergency department.
A high-dose sublingual tablet may be very useful in the treatment of emergency patients.
Abstral may be specially useful in treating children with severe pain.
–
So, what about overdose?
The goal of treating this overdose is a patient who is breathing adequately. Breathing adequately may be much slower than the 18 – 20 Breaths Per Minute that we mistakenly believe is normal, and therefore appropriate necessary for everyone.
The goal is not to take this over-medicated, but alive patient and completely reverse the fentanyl. If we do reverse the Abstral, then the patient is awake and in severe pain and not likely to respond to the small amount of opioids we carry, even if we carry 50 mg morphine or 500 mcg fentanyl.
We just completely reversed a dose that is probably larger than what we carry. If we do try to then treat the pain, what happens when that completely reversed dose of opioid kicks back in as the naloxone wears off?
The goal is an adequately breathing patient.
Adequate is a very subjective term defined by the patient.
–
Footnotes:
–
[1] FDA approves opioid analgesic to help cancer patients manage pain – Enrollment in REMS program required for health care professionals
FDA Press Release
For Immediate Release: Jan 7, 2011
Media Inquiries: Shelly Burgess, 301-796-4651, shelly.burgess@fda.hhs.gov
Consumer Inquiries: 888-INFO-FDA
FDA Press Release
–
[2] Abstral (fentanyl) immediate release SL tablets
FDA Label
PDF of FDA Label from FDA
.



I totally agree, the FDA needs to take on a new paradigm as far as dosing by weight. Many children present with BW (in these days with 50% of the population obese) as adults, thus subtherapeutic doses can occur, in every therapeutic category. In regards, to this medication being a controlled mediation, there is such a stigma and lack of clinicans really knowing when to employ good pain mgmt. There is a also a concern of promoting dependance and tachyphalyxis, Althoufh legititmate, it often leaves the pt with many breakthrough pain and a very poor quality of life. Moreover, in situations where there is hospice situation, an element of decreased rate of respiration is not the worse thing, in this patient cohort, there tends to be increased anxiety and the ultimate goal is palliative care. This additon would help, since some pts can not tolerate MSO4 and may have hemodynamic status, where fentanyl has a more favorable profile to that regard. I agree with your statements about overdoses and its role in the ED, most likely they have not done any studies in the setting, does not mean they will not do that, many medications are used off-FDA usage. Mark Albert- Pharmacist (Consultant for NYC REMSCO)
Mark Albert,
That shouldn’t be a problem, since this is only approved for those already dependent. This is one of the reasons the concern about addiction is a bit absurd.
I expect that this will occasionally be used in ED (Emergency Department), particularly for patients with cancer experiencing breakthrough pain. Too many of them end up in the ED because they do not have any better options, or because they are not aware of having any better options.
The main obstacle to use in the ED is –
This may prevent use in the ED. Especially since the approval specifically states that it is inappropriate for use in the ED.
Please, please, when making guidelines for this drug allow the EMT’s to dose to effect, not to weight, or standard maximum doses. Tolerances vary so much…perhaps basing the initial dose on their currently prescribed, ineffective dose would be allowable.
If ur local protocols allow to titrate, i agree
Anonymous,
This is not a drug that is being added to EMS protocols. This is a drug that is given in doses no smaller than 100 mcg, so not inappropriate for severe pain, but not likely to be used by EMS, or even doctors in the emergency department, any time soon.
canoehead,
This is not a drug that is being added to EMS protocols. This is a drug that is given in doses no smaller than 100 mcg, so not inappropriate for severe pain, but not likely to be used by EMS, or even doctors in the emergency department, any time soon.