The FDA (Food and Drug Administration) has come up with some new restrictions on acetaminophen in prescription medications and a new black box warning label.
[youtube]1xy73WK0YU8[/youtube]
–
In addition, a Boxed Warning highlighting the potential for severe liver injury and a Warning highlighting the potential for allergic reactions (e.g., swelling of the face, mouth, and throat, difficulty breathing, itching, or rash) are being added to the label of all prescription drug products that contain acetaminophen.[1]
What is the wording of the Black box[2] warning?
I don’t know. The video and the paragraph above are the extent of the information I could find. The labels do not seem to have been updated to include the black box warning. What it should state is something similar to what is in the video.
–
Acetaminophen is widely and effectively used in both prescription and over-the-counter (OTC) products to reduce pain and fever. It is one of the most commonly-used drugs in the United States. Examples of prescription products that contain acetaminophen include hydrocodone with acetaminophen (Vicodin, Lortab), and oxycodone with acetaminophen (Tylox, Percocet).[1]
And what effect will this have on OTC products?
OTC products containing acetaminophen (e.g., Tylenol) are not affected by this action. Information about the potential for liver injury is already required on the label for OTC products containing acetaminophen.[1]
Does anyone read the label on OTC products?
Probably only a very small percentage of patients. Most of these may be new parents wanting to make sure they do not give the wrong dose to their baby.
Will any older patients (over 30) start to read the label of OTC acetaminophen?
Probably only those who caught a news report on this.
What kind of effect will this have on toxicity/overdose and liver failure/death?
Although the present study identified age as a significant independent risk factor of paracetamol hepatotoxicity, the underlying mechanisms by which age increases the risk remain unclear, but are most likely multiple. Firstly, older individuals were more likely than younger individuals to develop FHF from paracetamol overdose. There is no evidence to suggest that paracetamol metabolism dramatically differs with age.15 Possibly, younger individuals may simply tolerate more extensive liver injury due to having a larger functioning liver cell mass prior to the overdose.16 This mechanism may be supported by the observation from the present study that the extent of hepatic injury, estimated by peak ALT, actually tended to be higher (p=0.07) in younger than in older individuals whereas hepatic dysfunction estimated by INR was significantly more pronounced in the older age group. Alternatively, younger individuals may better compensate for acute hepatic dysfunction (for example, via a higher capacity for extrahepatic metabolism of toxic substances such as ammonia which may be substantially metabolised by striated muscle tissue).29[3]
*Paracetamol is the name for acetaminophen outside of the US (both are generic names). OLT is Orthotopic Liver Transplantation. ALT is ALanine Transaminase. INR is International Normalized Ratio.
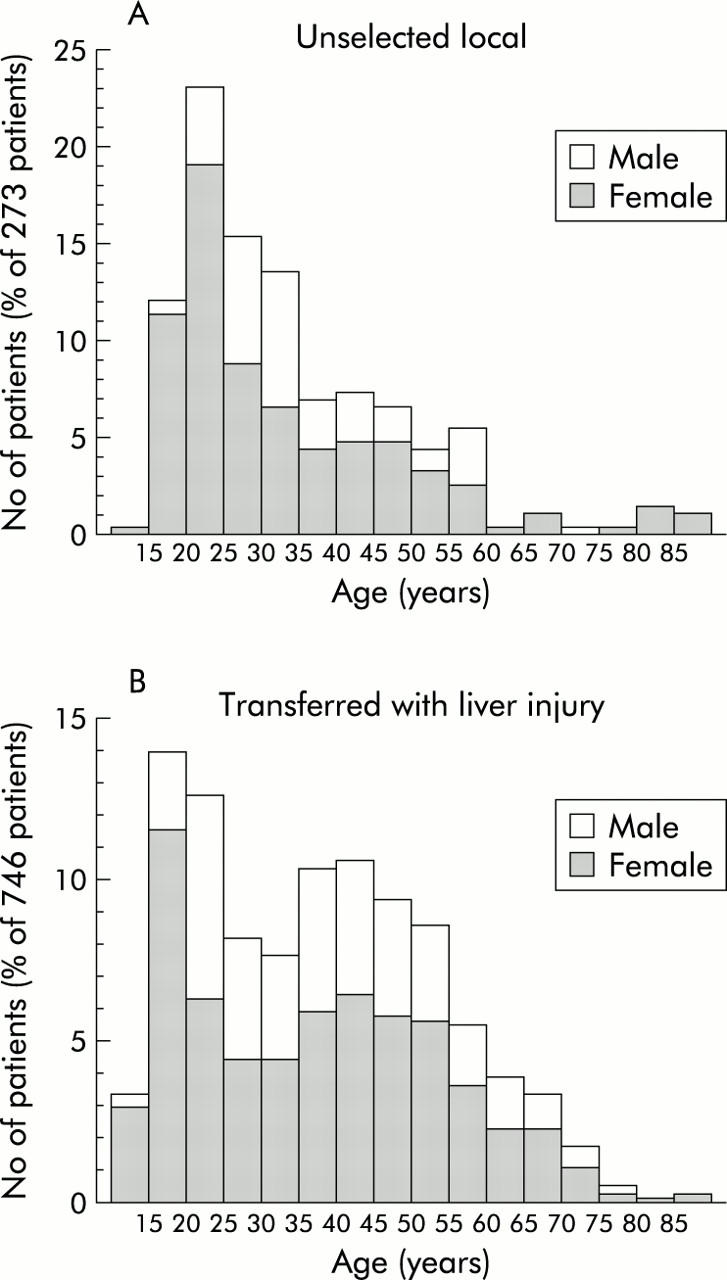
Figure 1[3]
Look at the number of cases of overdose. Then compare that with the number of cases of liver failure and the number of deaths. The lines extending above and below the graph bars indicate the 95% CI (Conficence Interval).
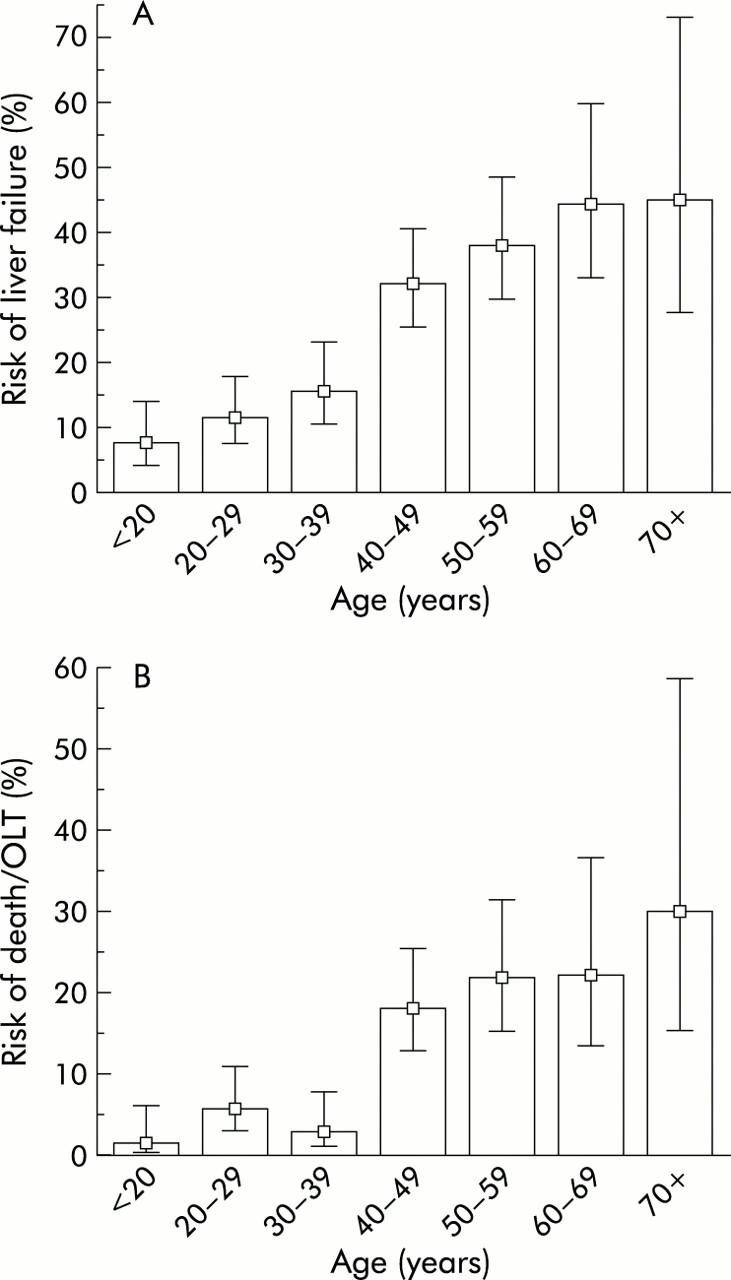
Figure 3[3]
Next look at the incidence of alcohol abuse.
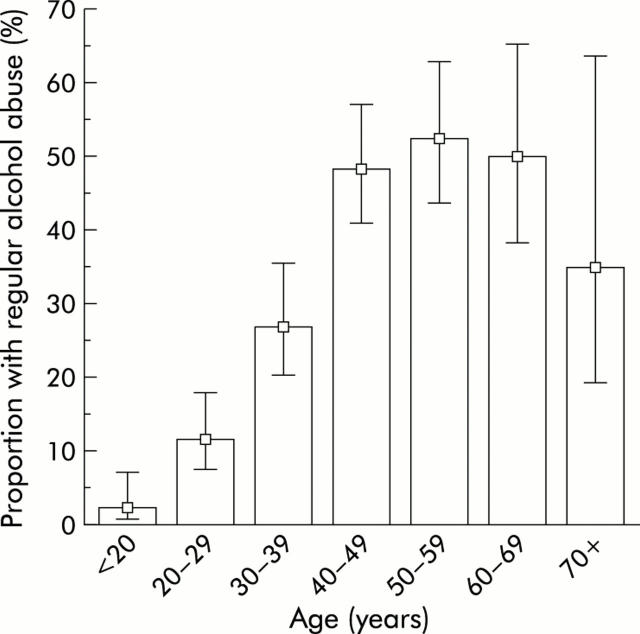
Figure 4[3]
Another factor is the delay from the time of ingestion of acetaminophen/paracetamol to the time of treatment with N-acetylcysteine in hours.The alcohol abuse drops off a little in the 60s and a lot in the 70s. The time to treatment keeps increasing with age.
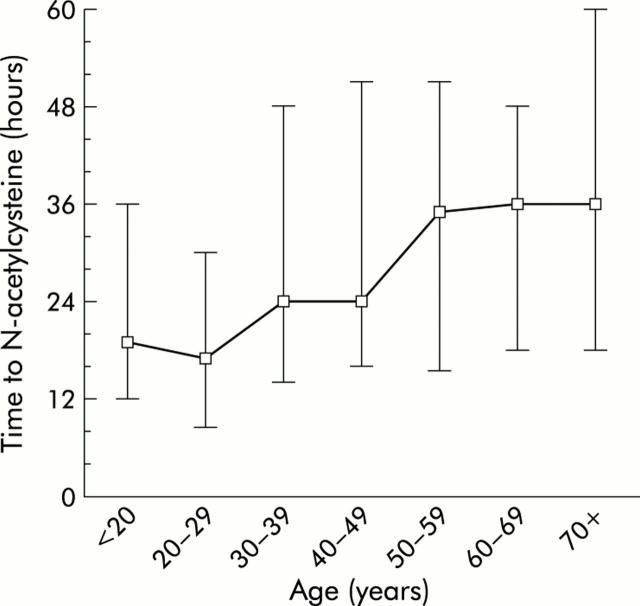
Figure 4[3]
The time to treatment much more closely matches the liver failure and death patterns. As the rate of alcohol abuse decreases, does the rate of liver failure or death decrease, or even stop increasing? No. Does this mean that the effects delay to treatment have a much greater impact in that age group, rather than an indication that alcohol has a modest effect or no effect?
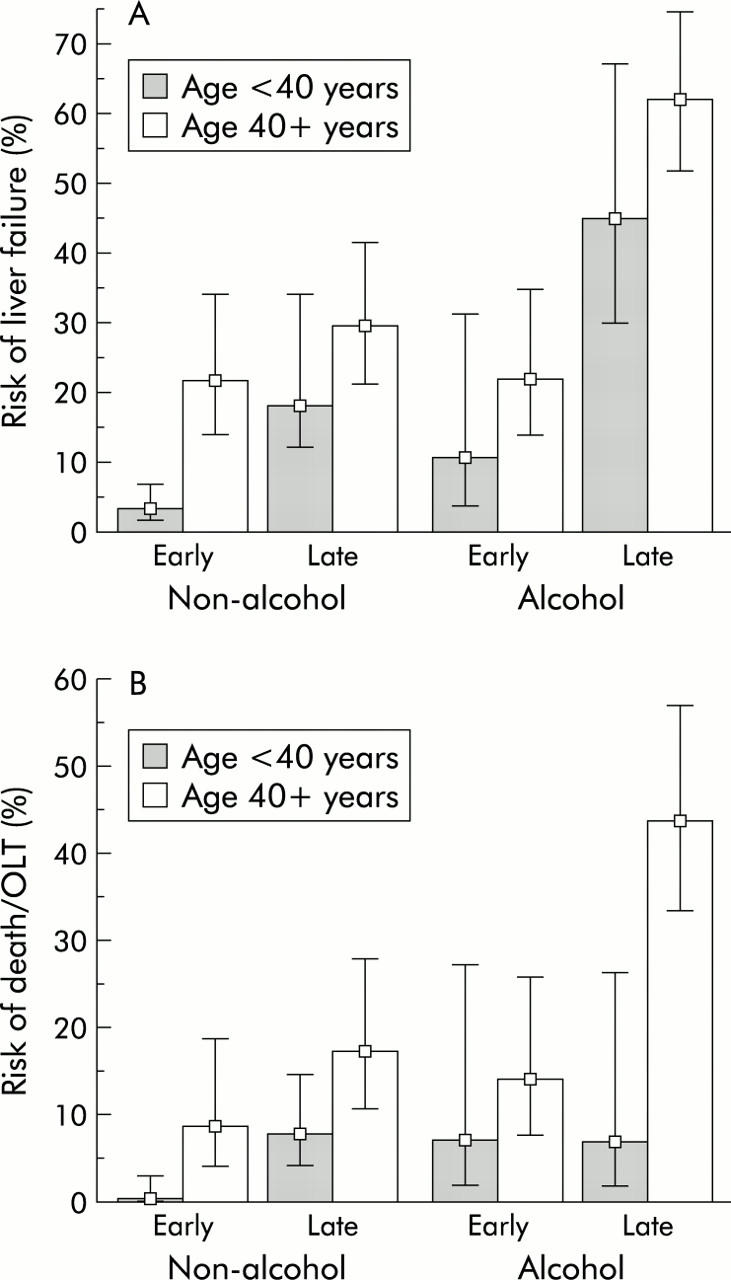
Figure 6[3]
No.
This final graph makes it clear that the effects of alcohol more than double the rates of liver failure and death.
Another interesting point is that the death rate in the under 40 year olds is flat, except for those who are treated early and do not abuse alcohol (for them it is about zero).
What about other factors, such as the dose of acetaminophen/paracetamol?
In order to establish the independent risk associated with age, a multivariate analysis using “age 40 years” together with known or suspected risk factors of paracetamol induced hepatotoxicity (sex, weight, quantity of paracetamol, “time to NAC”, regular alcohol abuse, acute alcohol co-ingestion, acetylsalicylic acid co-overdose, benzodiazepine co-overdose, and opioid co-overdose) as independent variables was performed.14,22 In this logistic regression analysis, the three major risk factors were “time to NAC”, regular alcohol abuse, and “age 40 years” (table 2 ).[3]
Are the new FDA rules likely to change the alcohol consumption or time to treatment for people ingesting toxic levels of acetaminophen?
Probably not.
–
Footnotes:
–
[1] FDA Drug Safety Communication: Prescription Acetaminophen Products to be Limited to 325 mg Per Dosage Unit; Boxed Warning Will Highlight Potential for Severe Liver Failure
FDA Safety Announcement
1-13-2011
FDA Safety Announcement
–
[2] Black box warning
Wikipedia
Article
–
[3] Age and paracetamol self-poisoning.
Schmidt LE.
Gut. 2005 May;54(5):686-90.
PMID: 15831917 [PubMed – indexed for MEDLINE]
Free Full Text with link to Free Full Text PDF from PubMed Central
.



I always assumed the acetaminophen (APAP) was in there to tacitly help discourage people from taking too many of theses opiod/APAP combos, in addition to increasing the analgesic effect of the medications. I’m curious to see if folks start popping even greater quantities of Percocet since there’s less chance of killing their livers.
On the other hand, these abusers who take analgesics for fun also tend to be slightly less informed when it comes to health matters, and may not realize the effect the acetaminophen could have on their bodies, especially when combined with alcohol (or just as likely, they are aware and don’t care). Perhaps, in the end, the issue will balance out with less harm from APAP induced hepatotxicity and more harm from opiate overdose.
Or maybe the FDA really just has the majority of patients in mind; the ones who don’t abuse these medications and just end up building up high acetaminophen levels from their chronic use to treat high levels of pain.
The point I’m moving towards is that it’s possible this FDA action could help increase the safety of these medications, but I won’t be the least bit surprised if five or ten years from now, we realize that simply reducing the quantity of acetaminophen in these combo pills wasn’t the way to go about mitigating the harm these meds can do. The problem probably isn’t the level of Tylenol in the pills, but the number of pills individuals take and the risk factors that increase the ill effects of the medications. If you have someone in pain who is just running through bottles of Vicodin, they need better pain management, not the same meds with slightly less APAP. Or, if you have someone going through an equal amount of pills, but for recreational purposes, they don’t need less Tylenol in their system, but less ability to get high quantities of a controlled substance so easily. And if either of these patients drink, they need to be well aware that they will end up needing a new liver (and probably won’t get one).
I’m mostly rambling here, but I just wanted to toss out some broad ideas in addition to your much more focused posting on the effect of this new limit. As always, it was a well reasoned and supported view of the issue, thanks for the continued excellent work on this blog.
NAPQI (N-acetyl-p-benzo-quinone imine) is the MECHANISM OF ACTION of Acetaminophen, Paracetamol, Tylenol etc.
Yes it’s the minor yet significant alkylating TOXIC metabolite which is the actual pain KILLER!
And that’s exactly how is works!
By killing everything it touches!
The pain receptors in the brain (neurons and glial).
Spinal TRPA1 receptors, alkylizing the spine, becoming the cause of severe lower-back and knee pain.
Use for over 10 days will start the path of destruction …
BEWARE … THEY DON’T CARE WHAT HAPPENS TO YOU … THEY HAVE BILLIONS INVESTED … MONEY OVER PEOPLE EVERY TIME …
They even use it for months on the elderly, calling it ‘Best Interest’ not letting you know it’s full title is
‘Best Interest – End of Life’!
Evil – pure EVIL!
Mary,
Many natural treatments are also toxic – even more toxic than NAPQI.
Fortunately, the body makes glutathione, which detxifies NAPQI. This is similar to the alcohol dehydrogenase that detoxifies alcohol.
There is nothing wrong with killing pain.
–
That is not true.
If you want to make these claims, provide some evidence.
You are just making a fool of yourself.
–
Again – provide some evidence.
–
This is not true.
On the other hand, it does contradict your earlier claims that NAPQI works by killing the brain cells. Acetaminophen works much more quickly than ten days.
Which of your lies do you want us to believe?
–
Now it is clear – you are a conspiracy theorist.
Go push your alternative medicine/natural medicine fraud elsewhere.
Stop abusing patients with your fraudulent scare stories, you quack.
.