In response to A Whole 2 mg of Morphine – All At Once, Chris from EMS Patient care advocate One wrote –
Severe pain + 2 mg morphine = severe pain.
Ah, I am sorry about that.
Though is the “severe” necessary?
Is the use of the word severe necessary?
Is it essential to make my point?
Maybe for some people only severe pain is considered treatable. If pain management were easy to understand, it would not require so much explanation and the numbers of under-treated patients would be limited to those who are refusing treatment (which I think means that they are not under-treated). This does not appear to be the case.
Appropriate pain management for moderate pain or for severe pain does not appear to be anywhere in the predictable future for EMS in general.
–
If 2mg is equal to a placebo, perhaps you mean ANY pain treated with 2mg IV morphine (excluding special patient circumstances) would still have the same amount of pain?
I found it to be an interesting quote. I again apologize for leaving part of it out.
No.
Placebos appear to have their greatest effect on pain. Sometimes giving something insignificant will result in some of the pain going away. Sometimes giving something insignificant will result in all of the pain going away. With placebos and with doses that are not significant, it isn’t the dose that was effective, but the suggestion. Placebo is less effective than appropriate opioid doses for moderate or severe pain.
–
Do we not provide pain management to moderate pain?
Yes, we do – just with more moderate doses.
These doses should be repeated until the patient does not want any more pain medicine or until the patient has side effects suggesting that further doses may mot be not safe. This part is the same as with severe pain. The difference is the initial dosing. I have started with 10 mg morphine/100 mcg fentanyl for average sized people with severe pain. That is higher initial dosing than I would recommend for treating moderate pain.
–
How much Morphine is needed to treat someone with “real” pain who has a high tolerance to narcotics?
Whatever doses we started with should be repeated until the patient does not want any more pain medicine or until side effects suggest that further dosing is not safe.
There is no specific mg dose that is enough.
There is no specific mg dose that is too much.
The only way to determine if something is enough/too much is by the response of the patient. We must be able to assess to be able to titrate.
–
Do they not deserve proper dosing just because they require higher than the “normal magic pain relief” dose?
They do require proper dosing.
When I have treated patients with Duragesic patches, I have given very large mg/kg total doses, when I could get appropriate orders from medical command.
–
I point out the options to the patient. I can call a different hospital for orders and possibly receive appropriate orders. I can transport the patient to a different hospital. I can do both.
Good point. I would certainly need to put some big boy pants on. However, I have two hospitals within 20 min. Any others, we are talking about over an hours travel time. I would really be putting myself in the spotlight at the state level doing this.
I have a lot of hospitals to choose from.
I have also been told that calling other doctors for appropriate orders is bad.
This is just the typical insanity of medical command permission requirements. We are threatened with punishment for ethical behavior. We are threatened with punishment for not abusing patients.
I have done this a few times, but I have never been punished for this. An alternative is to call a hospital where I know that the medical command doctor on duty is aggressive with pain management and ask for orders from that doctor.
One hospital where I used to work had some doctors who would give us orders for aggressive dosing – as long as we were taking the patient to a different hospital.
The first rule of medical command permission requirements is to know which doctors are answering the medical command phone at which hospitals.
The second rule of medical command permission requirements is to know what mood the doctors are in. Some are very moody, while others do not appear to vary their orders based on their moods.
Medical command permission requirements do not exist to protect patients.
Medical command permission requirements do exist to make medical directors comfortable authorizing incompetent medics to treat patients.
If medical command permission requirements were about patient care, nobody would object to a medic calling for a second opinion.
If medical command permission requirements were about patient care, the orders would not vary so much from doctor to doctor. A Magic Eight Ball is more consistent.
–

–
Some emergency physicians certainly do appear to be afraid of appropriately treating patients with pain. Or maybe they just do not understand pain management.
I’m not sure all ED doctors that cover the medical control line have any training on being medical control and seem to have no training in pre-hospispital pain managment. Actually I’d say a lot of pre-hospital medicine all together is not understood. Some Docs are great and took interest in what we do and take the time to understand.
Yes.
–
I can see how it could make a doctor feel vulnerable to give the online order, but it’s so easy to put up a shield “out of sight, out of mind”.
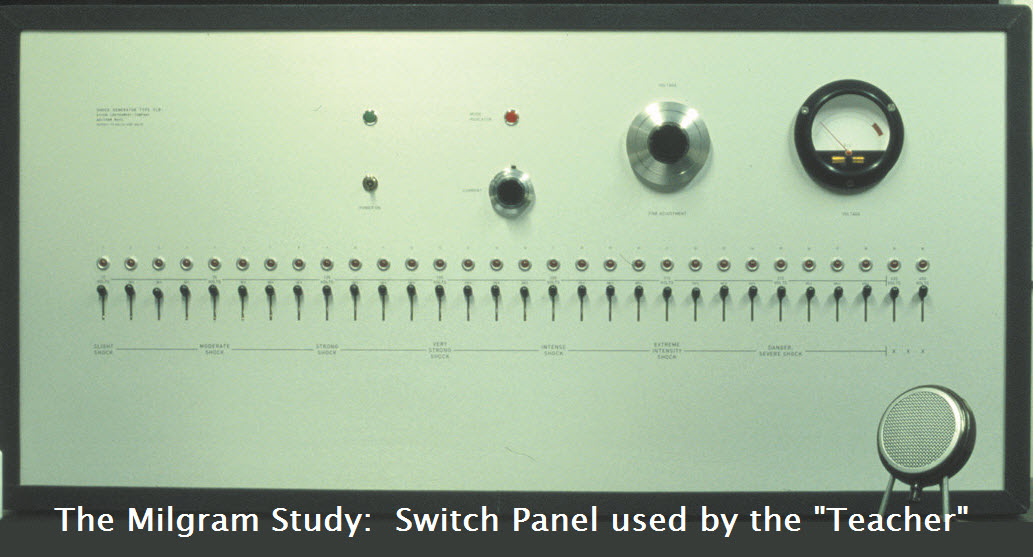
This was studied very well by Stanley Milgram. When the person delivering the shock to the subject victim could not see the subject victim, people were more likely to give a shock that was labeled as DANGER – SEVERE SHOCK. We paramedics are not much different. We allow doctors to order us to cause severe pain to patients when the doctors order us not to treat severe pain or when doctors order us to under-treat severe pain. We give up too easily when it comes to ethics.
Are we acting any differently from those delivering unnecessary shocks when we cause unnecessary pain?
–
–
It is admitted that a lot of doctors in this area really don’t know EMS or how we operate exactly (they just don’t have any training on how to be medical control, who knows).
Also it seems forgotten that bouncing down the road, carefully or not, provokes pain-a lot. They aren’t laying still in a hospital bed. In my short experience as a Medic patients treated with Morphine or Fentanyl the pain relief wears off much faster in the pre-hospital setting than when the same dose is given in the hospital setting.
I don’t know if opioids wear off any more quickly, but there is much less painful stimulus in a hospital bed, than when bouncing down bumpy roads, lying on a thin mattress placed over the rear axle of a truck that is not treated gently.
Some doctors understand pain management. Some doctors do not seem to understand what pain is. Some doctors act as if ethics and responsibility only apply after the doctor’s patient is seen by the doctor.
.



What about all the natural drugs! all opiates come from poppies! & if you eat enough natural poppy seeds you get the effects! poppy seeds are not man made!
morphine side effects,
The distinction between man made treatments and all natural treatments is worthless.
Should we treat people with the wonderful all natural cyanide?
What about all natural anthrax?
We could use some all natural bleeding to try to get the humours back in line.
All of these are all natural.
None of these are good for patients.
There is nothing about being all natural that makes a treatment better. Not more effective. Not safer. Not faster. Not fewer side effects. Nothing.
What kind of dose of poppy seeds would be effective in reducing severe pain?
I have eaten food with poppy seeds. I did not notice any effect, even though there were dozens of poppy seeds.
100 all natural seeds?
1,000 all natural seeds?
1,000,000 all natural seeds?
1,000,000,000 all natural seeds?
What kind of evidence do you have of any benefit of giving poppy seeds?
Maybe people just say they feel better to get you to stop feeding them so many seeds.
Would the patient end up needing surgery for a bowel obstruction – assuming the patient ever consumed enough poppy seeds? Would that be an example of a good all natural treatment?
Should we carry a hookah and have the patient smoke some all natural opium?
Why do you claim that there is something better about being all natural?
.
This article is good enough for pain Management at the initial stage. This post is too informative and nice. Thanks for the Post.