
Perhaps, you have watched all of the parts of Saw and wished that you could have some of that kind of fun, too. Even though we are supposed to be having the opposite effect on patients, some of us do cause that kind of pain and psychological abuse.
Dr. Weingart gives us a piece of his mind on this topic in Pain and Terror as Effective Pressors.
–
Does this go well with scrubs, or with an EMS uniform?

–
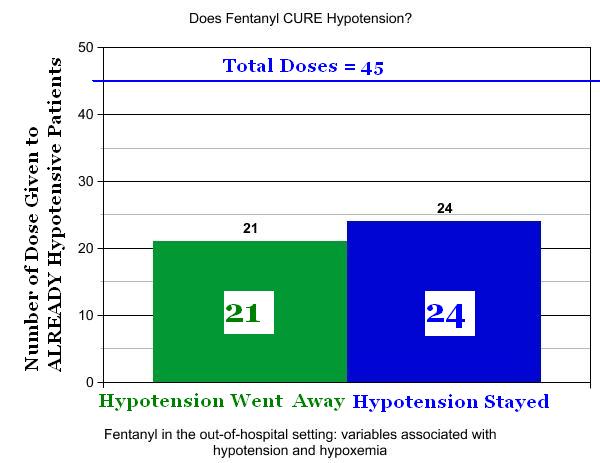
But what about the hypotension and hypoxia that occur with fentanyl?
–
Click on images to make them larger.[1] [2]
–
–
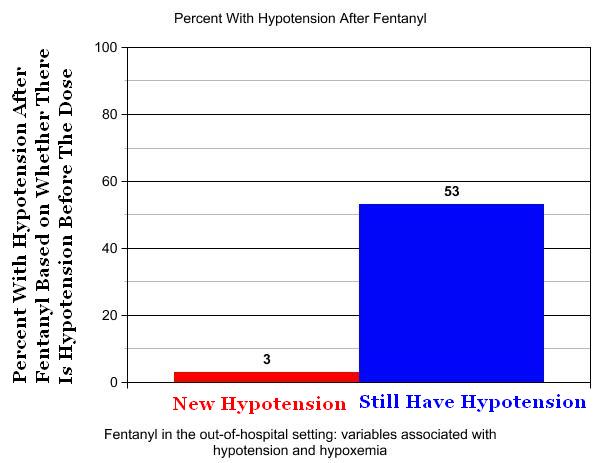
There is a 97% chance that, after administration of fentanyl to a critical trauma patient who is not hypotensive, the patient will still be not hypotensive.
There is a 47% chance that, after administration of fentanyl to a critical trauma patient who is hypotensive, the patient will stop being hypotensive.
If we did not have so much anxiety about fentanyl, we might consider making it the standard of care for hypotension following trauma.
–
Should we be double-teaming these patients with both pain and the terror of awareness during intubation with a long-acting paralytic? It probably isn’t any worse than what the traumatically paralyzed patient experiences with intubation, but that should only encourage us to be more aggressive with pain management for these patients. This is not an excuse to be tolerant of iatrogenic pain and anxiety.
Pain management in EMS seems to keep improving, but we still have a long way to go.
Pain management in the ED (Emergency Department) seems to keep improving, but we still have a long way to go.
I currently do have a protocol that allows me to give post-intubation sedation. This was only added to my protocols in the past 5 years, but it is a start. Before that, medics had to be aggressive enough to ask for medical command permission for a treatment that was outside of protocol. Treatments that are outside of protocol are discouraged.
–
The problem with post-intubation pain (and the expected agitation that goes with pain) this pain management sedation is not a recent development.
In an earlier podcast, Dr. Weingart describes the problems with using sedatives, rather than pain medicine, for post-intubation PAIN.
EMCrit Podcast 7 – Sedation Tirade – and listen to his other sedation podcasts.
Why do we think that a patient does not have pain unless that patient is writhing in pain?
With a paralytic on board, especially a long-acting paralytic, and even more so with a large dose of a long-acting paralytic, these patients will not writhe.
This brings up some questions –
How much evidence do we need that many of our patients are in a lot pain?
How easy is it to ignore the severe pain of our patients?
–
I do have one criticism.
The dose of sarcasm could be increased. This is no time to be stingy with the sarcasm treatment. I could be wrong.
Go listen to the brief Wee podcast and decide for yourself.
–
Footnotes:
–
[1] Fentanyl in the out-of-hospital setting: variables associated with hypotension and hypoxemia.
Krauss WC, Shah S, Shah S, Thomas SH.
J Emerg Med. 2011 Feb;40(2):182-7. Epub 2009 Mar 27.
PMID: 19327928 [PubMed – in process]
Full Text PDF Download at medicalscg.
Fentanyl Study: EMS Research Episode 9
EMS Research Podcast
Podcast page
–
[2] Chart Version – Fentanyl in the out-of-hospital setting: variables associated with hypotension and hypoxemia
Sun, 05 Jun 2011
Rogue Medic
Article
–
.



{kind=link}
I’m not in your industry at all, but listening to the podcast gave me chills. How is it that Dr. Weingart even needs to point that out to people? Shouldn’t it be obvious to people have having a chunk of plastic shoved down your trachea is both painful and scary? I imagine myself in a situation like that and I’d be begging for pain control.
Of 3% of patients given fentanyl that became hypertensive, could it be possible that they were under medicated?
I have said for years, since Vec and Roc have been added to ambulances with the RSI protocols, EMS needs a long acting sedative or dissociative that is safe to use with hypotension. Versed is good when hypotension is not an issue and Ativan with Fentanyl is adequate with hypotension but, Ketamine or Propofol is better.
We have Succs for the intubation and in all reality if we had the proper meds for long term sedation we would not need to use our Vec but, medical directors would rather give us half the tools for patient care than allow us to properly treat the patient. Makes no sense to me that I can use a long acting paralytic but, not a short or long acting sedative that is appropriate for patient condition.