What prevents us from treating pain appropriately?
Actual adverse effects of pain medicine or unwarranted anxiety, due to exaggerated fears of potential adverse effects of pain medicine?
–
In 1999, the Emergency Medical Services Outcomes Project identified prehospital pain relief as a priority outcome and noted that it is one of the most high-impact prehospital interventions that can be performed on the majority of patients.3 [1]
Pain management is important. Unfortunately, EMS and emergency medicine have been better at coming up with excuses for not treating pain, than we have been at coming up with good protocols that encourage treating pain.
–
Our hypothesis was that a single dose of intravenous fentanyl administered in the prehospital setting would have no detrimental effect on the shock index of initially normotensive adult trauma patients.[1]
If we appropriately assess our patients, give reasonable doses of fentanyl (or any other pain medicine), is there any good reason to expect that there will be any harm to patients?
If we cannot appropriately assess our patients, what kind of incompetence justifies authorizing us to work as paramedics?
–
The protocol change allowed paramedics to administer a single 100 µg dose of fentanyl to adult trauma patients being transported “Code 10” (e.g., lights and sirens) to the hospital without a call to the medical command center. No other opioid was allowed for pain management in this population. Before the protocol change, medical command approval was required before administration of fentanyl.[1]
I see this as even more evidence that medical command permission requirements have nothing to do with protecting patients.
When medical command permission was required, pain management was rare.
–

–
After the protocol change patients were almost 6 times more likely to receive fentanyl.
The harm of medical command permission requirements is not controlled for, nor is it a hypothesis of the study. If this does reflect the way that medical command permission requirements discourage, or prevent, appropriate patient care, that raises a question –
How can we justify continuing to allow our patients to be harmed by medical command permission requirements?

–
Inclusion criteria were (1) age ≥ 18 years; (2) systolic blood pressure (SBP) >90 mm Hg; (3) Glasgow Coma Scale (GCS) score ≥13; and (4) emergent trauma transport to Denver Health Medical Center. Emergent trauma was defined as any “Code 10” (e.g., lights and sirens) transport to the hospital. Exclusion criteria were pregnancy and imprisonment.[1]
Pain is not listed as an inclusion criterion.
Severe pain? Moderate pain and severe pain? Abdominal pain? What is permitted on standing orders?
–
The outcome was the initial ED shock index (defined as the heart rate divided by SBP). As pain relief from fentanyl would typically result in a decrease in both heart rate and blood pressure, the shock index was chosen as a composite outcome for its ability to reflect, as a single dependent variable in a multivariable model, abnormal changes in heart
rate and blood pressure.[1]
This may be a better way to assess vital sign changes than just looking at blood pressure, but is this part of what is used during anesthesia or procedural sedation to assess vital signs?
What if the patient is hypotensive before fentanyl, then receives fentanyl? What if some pain relief produces the expected decrease in heart rate, but the same pain relief also produces an increase in blood pressure?
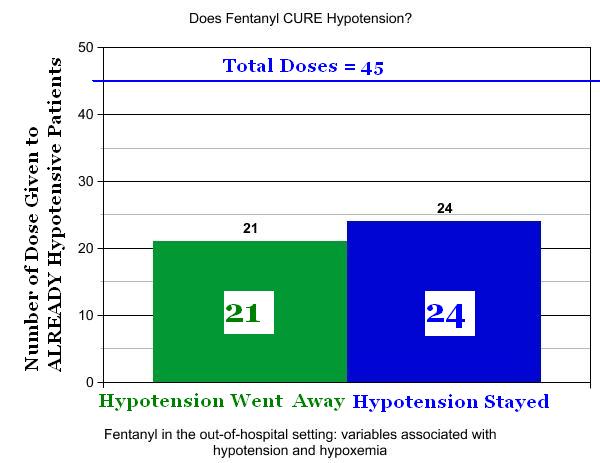
This study’s protocol would not permit giving fentanyl to hypotensive patients, but that study has already been done –
–
Click on images to make them larger.[2] [3]
–
In 47% of cases of administration of fentanyl to already hypotensive trauma patients, the hypotension went away after fentanyl.
Why aren’t we doing larger studies of giving fentanyl to hypotensive patients?
Why are we withholding fentanyl from hypotensive patients?
What if . . . ?
What if we behave intelligently and actually find out?
Perpetuating myths and traditions is bad for patients.
We need to stop the defenders of tradition and mythology from harming our patients.
–
–
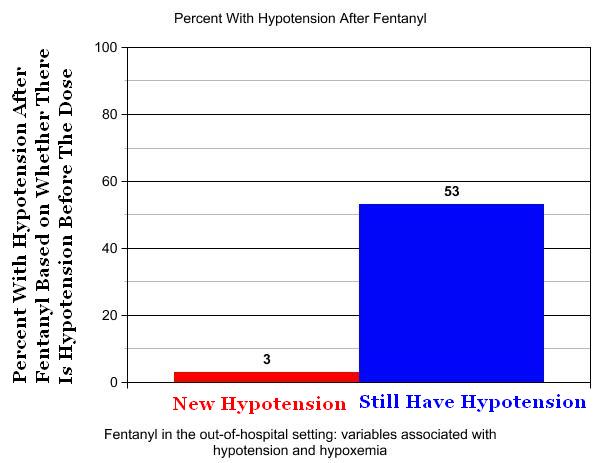
There is a 97% chance that, after administration of fentanyl to a critical trauma patient who is not hypotensive, the patient will still be not hypotensive.
There is a 47% chance that, after administration of fentanyl to a critical trauma patient who is hypotensive, the patient will be not hypotensive.
If we did not have so much anxiety about fentanyl, we might consider making it the standard of care for hypotension following trauma.
A total of 1,669 patients met criteria for inclusion during the study period.[1]
This is one of the problems with not fully describing the criteria. Did all of these patients have pain that met the criteria for administration of fentanyl? If so, then giving fentanyl to only 217 patients (13% of 1,699) is horrible.
–
Seven patients had an initial ED SBP <90 mm Hg, and all were included in the control group.[1]
Would fentanyl have prevented those cases of hypotension?
–
Footnotes:
–
[1] Safety of prehospital intravenous fentanyl for adult trauma patients.
Soriya GC, McVaney KE, Liao MM, Haukoos JS, Byyny RL, Gravitz C, Colwell CB.
J Trauma Acute Care Surg. 2012 Mar;72(3):755-759.
PMID: 22491566 [PubMed – as supplied by publisher]
–
[2] Fentanyl in the out-of-hospital setting: variables associated with hypotension and hypoxemia.
Krauss WC, Shah S, Shah S, Thomas SH.
J Emerg Med. 2011 Feb;40(2):182-7. Epub 2009 Mar 27.
PMID: 19327928 [PubMed – in process]
Full Text PDF Download at medicalscg.
Fentanyl Study: EMS Research Episode 9
EMS Research Podcast
Podcast page
–
[3] Chart Version – Fentanyl in the out-of-hospital setting: variables associated with hypotension and hypoxemia
Sun, 05 Jun 2011
Rogue Medic
Article
–
Soriya GC, McVaney KE, Liao MM, Haukoos JS, Byyny RL, Gravitz C, & Colwell CB (2012). Safety of prehospital intravenous fentanyl for adult trauma patients. The journal of trauma and acute care surgery, 72 (3), 755-759 PMID: 22491566
.



Interesting study, thanks for publicizing it.
True, it has the significant limitation that so much EMS research does – the “before and after” study, and the myriad confounding factors in such studies. For example, as the authors admit, “A selection bias was potentially present for paramedics deciding which patients received fentanyl.” Probably that should be the very next study, explaining why one paramedic gave fentanyl to one patient, and not another, given the same injury score, shock index, etc.
One more reference you might find useful – or perhaps you already have it. Stephan Thomas, in Boston, wrote a great review of trauma analgesia (http://www.ncbi.nlm.nih.gov/pubmed/17997072). He takes on all the historic prohibitions that have held back analgesia in that context: the fear of altering the mental status exam, the change in the abdominal exam, and the potential for hypotension. He highlights much evidence that is line with the Krauss study, as well as Soriya, not to mention your own perspective.
Regarding medical command requirements, I believe that analgesia should be standing order. However, I’m not sure that the sole act of making it standing order will change EMS provider behavior to a large extent. Soriya et al. gloss over what other formal interventions or education accompanied the change in protocol, let alone what cultural, or informal, changes occurred. I rather doubt that the protocol revision was made without any roll-out, education, or promotion.
As for the picture of the medical control physician on the phone, I generally shave before my shifts!