
–
Continuing from Part I of my examination of the topic of bad evidence-based guidelines raised by Dr. John M –
If I was a professor of Medicine and not just a blogger, my bottom-line message would be simple:
Use the fury of medicine sparingly. Heck, you could even suggest a time out before writing e-prescribing a medicine.[1]
Fury?
A reference to epinephrine (stress, heart failure, and heart attack in a syringe)?
Our evidence-based guidelines should be written conservatively. The problem is not with the evidence, but with the inappropriate weight given to weak evidence. We base standards of care on weak evidence (as with ACLS – Advanced Cardiac Life Support), or on evidence that is irrelevant (as with immobilization on a backboard). We are fools. We make guidelines out of the shoddy material we have, rather than having the guidelines wait until there is valid evidence to make a good foundation for patient care.
The evidence needs to fit the patients. Procrustes would make a bad doctor, but he would love strict guidelines. We should not force the patients to fit the evidence.
Let’s look at the algorithm for VF (Ventricular Fibrillation)/Pulseless VT (Ventricular Tachycardia).
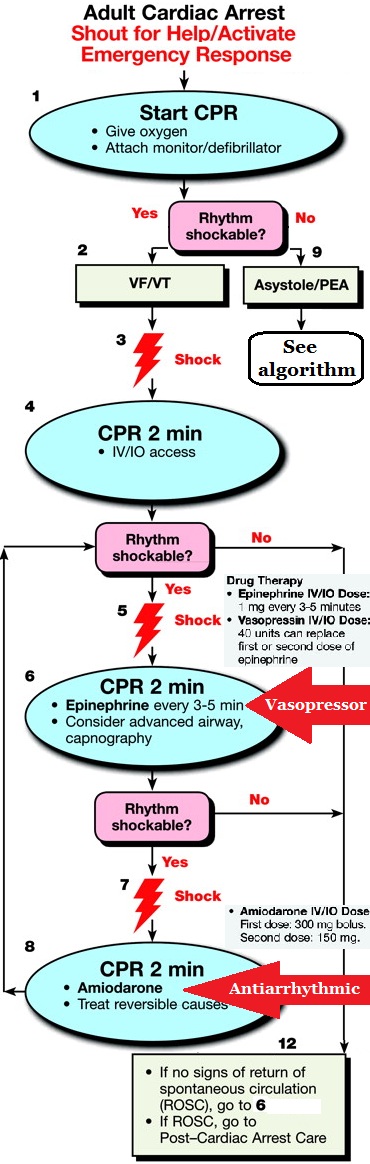
Click on image to make it larger.
Now let’s compare what is written in the ACLS guideline that produces the requirements for treating VF/pulseless VT with a vasopressor (epinephrine, and/or vasopressin, or norepinephrine, or phenylephrine) and an antiarrhythmic (amiodarone, or lidocaine, or magnesium).
It is reasonable to consider administering a 1 mg dose of IV/IO epinephrine every 3 to 5 minutes during adult cardiac arrest (Class IIb, LOE A).[2]
A mandatory step or just reasonable to consider?
Because the effects of vasopressin have not been shown to differ from those of epinephrine in cardiac arrest, 1 dose of vasopressin 40 units IV/IO may replace either the first or second dose of epinephrine in the treatment of cardiac arrest (Class IIb, LOE A).[2]
There are no alternative vasopressors (norepinephrine, phenylephrine) with proven survival benefit compared with epinephrine.268,281,282 [2]
This makes it seem as if epinephrine is better than these drugs, but is epinephrine better than nothing?
To date no placebo-controlled trials have shown that administration of any vasopressor agent at any stage during management of VF, pulseless VT, PEA, or asystole increases the rate of neurologically intact survival to hospital discharge.[2]
No treatment has been shown to be better than nothing.
Strike that. Reverse it. Does the meaning change?
Does it matter if we give epinephrine, or vasopressin, or norepinephrine, or phenylephrine? Not according to the way these guidelines are written, but maybe according to the way they are interpreted.
Has any drug been shown to be better than no drug for cardiac arrest?
Absolutely not.
What do we do with that information?
We ignore it and we give drugs.
Amiodarone may be considered for VF or pulseless VT unresponsive to CPR, defibrillation, and a vasopressor therapy (Class IIb, LOE B).[2]
Mandatory or may be considered?
But there is inadequate evidence to recommend the use of lidocaine in patients who have refractory VT/VF, defined as VT/VF not terminated by defibrillation or that continues to recur after defibrillation during out-of-hospital cardiac arrest or in-hospital cardiac arrest.[2]
there is inadequate evidence to recommend the use of lidocaine
Is that a recommendation?
Lidocaine may be considered if amiodarone is not available (Class IIb, LOE B).[2]
But, if we don’t have amiodarone (which doesn’t work) we can pretend that lidocaine is amiodarone. As long as we are giving treatments that do not work, does it matter which treatments we give?
A number of doses of magnesium sulfate have been used clinically, and an optimal dosing regimen has not been established. When VF/pulseless VT cardiac arrest is associated with torsades de pointes, providers may administer an IV/IO bolus of magnesium sulfate at a dose of 1 to 2 g diluted in 10 mL D5W (Class IIb, LOE C).[2]
Thus, routine administration of magnesium sulfate in cardiac arrest is not recommended (Class III, LOE A) unless torsades de pointes is present.[2]
What do we really need to know about antiarrhythmics?
There is no evidence that any antiarrhythmic drug given routinely during human cardiac arrest increases survival to hospital discharge.[2]
Nothing has been shown to be better than no treatment.
Does it matter if we give amiodarone, or lidocaine, or magnesium? Not according to the way these guidelines are written, but maybe according to the way they are interpreted.
Is this a fault of the guidelines of of those of us misinterpreting the guidelines?
Is this a fault of the evidence, and there is no evidence that any drug improves real survival, or a fault of the overly optimistic misinterpretation of weak evidence?
A huge problem with the way the evidence is interpreted is that the class and the levels of evidence are able to hide the most important factor – the distinction between surrogate endpoint evidence and survival evidence.
We usually base guidelines on surrogate endpoint evidence.
Surrogate endpoint evidence-based treatments kill.
Surrogate endpoint evidence requires confirmation with survival evidence, because surrogate endpoint evidence does not predict survival evidence.
Any standard of care guideline that does not have evidence of survival benefit needs to have an expiration date.
For example –
If there is no evidence of improved survival by the time of the next review of the guidelines, this treatment will be removed from the guidelines.
Cardiac arrest guidelines that require administration of epinephrine are NOT evidence-based.
Cardiac arrest guidelines that require administration of amiodarone are NOT evidence-based.
ACLS does NOT require administration of epinephrine or amiodarone for cardiac arrest.
Evidence-Based Medicine should not be blamed for violations of Evidence-Based Medicine.
–
PS – There isn’t any evidence that any kind of vascular access, ventilation, or airway intervention improves survival. These are purely unreasonable optimism-based treatments.
–
Footnotes:
–
[1] How much Medicine is enough?
Dr. John M
June 25, 2012
Article
–
[2] Medications for Arrest Rhythms
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Part 8: Adult Advanced Cardiovascular Life Support
Part 8.2: Management of Cardiac Arrest
Free Full Text from Circulation
.



[…] Too Much Medicine and Evidence-Based Guidelines – Part II – Tue, 03 Jul 2012 […]