The return of consciousness without the return of a pulse is still rare, but may be more common with our increased focus on high quality chest compressions. There is still no evidence that interrupting chest compressions, for anything other than defibrillation, improves outcomes.
Is this due to the consistency of the machine? Maybe. Maybe not. We do not have enough evidence to draw that conclusion.
Is this growing population really growing? Maybe. Maybe not. We do not have enough evidence to draw that conclusion, either.
It could be that with the ability to use a cell phone camera to record these instances, there is more credibility to the reports. There is a suggestion that this could be common.
Parnia et al. conducted a multi-year, multi-center, prospective study of the frequency of awareness during resuscitation by interviewing cardiac arrest survivors after discharge. They found 55/140 (39%) had perceptions of awareness of being alive and even memories that originated during that time.2 [1]
Should we be giving ketamine to these patients?
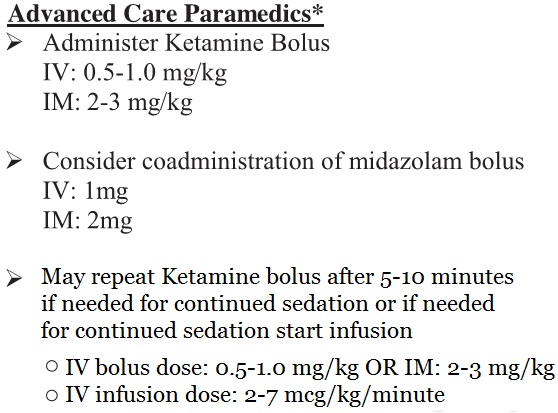
Nebraska CPR Induced Consciousness Sedation Protocol (from the PDF)[1]
We should find out how common it is for people to regain consciousness without regaining a pulse. This is clearly an experimental protocol that is not supported by evidence of improved outcomes that matter – just like all of the rest of cardiac arrest treatment that is not compressions or defibrillation.
RESULTS: The search yielded 1997 unique records, of which 50 abstracts were reviewed. Nine reports, describing 10 patients, were relevant. Six of the patients had CPR performed by mechanical devices, three of these patients were sedated. Four patients arrested in the out-of-hospital setting and six arrested in hospital. There were four survivors. Varying levels of consciousness were described in all reports, including purposeful arm movements, verbal communication, and resuscitation interference. Management strategies directed at consciousness were offered to six patients and included both physical and chemical restraints.[2]
6/1,997 is 0.3% – not anywhere near the 39.3% of 55/140, but it is still a large enough group that we should not ignore them.
Depression and anxiety following resuscitation are significant problems, so this might even be a way to help decrease those resuscitation side effects.
CONCLUSION:
One fourth of OHCA-survivors reported symptoms of anxiety and/or depression at 6 months which was similar to STEMI-controls and previous normative data. Subjective cognitive problems were associated with an increased risk for psychological distress. Since psychological distress affects long-term prognosis of cardiac patients in general it should be addressed during follow-up of survivors with OHCA due to a cardiac cause.[3]
The similarity to the outcome of STEMI (ST segment Elevation Myocardial Infarction) patients do not inspire confidence in this approach, but that does not mean that it should not be examined.
It is most important that we not make the mistake that has been made with ventilations, endotracheal tubes, extraglottic airways, antiarrhythmic drugs, pressor drugs, anti-acidosis drugs, antidote drugs, anti-hypoglycemic drugs, et cetera. We should insist that there be valid evidence of some sort of benefit before the ACLS (Advanced Cardiac Life Support) Committee of Failed Treatments adds this to the ACLS algorithms because of an abundance of wishful thinking.
This time will be different.
This use of ketamine is interesting. Ketamine is a sedative that should not depress vital signs, so it may do what we expect. There may be more benefit than harm, but there may be more harm than benefit, or there may be all harm and no benefit. We will not know until we have valid research.
We have added the other treatments without finding out if they improve outcomes. We continue to remove these treatments as we obtain evidence, because they have one thing in common – they don’t improve outcomes.
These treatments have increased the ignorance of those who work in EMS (Emergency Medical Services) and EM (Emergency Medicine). We keep convincing ourselves that we know what we are doing, but evidence keeps showing that we are lying to ourselves.
Maybe ketamine sedation during compressions will be beneficial. It is such a small patient population, that it will be difficult to study. Introducing a treatment without studying it will always be a mistake. Is Nebraska studying this? Probably, but it is not stated in the paper. Has this been approved by an IRB (Institutional Review Board)? I do not know.
–
Footnotes:
–
[1] CPR induced consciousness: It’s time for sedation protocols for this growing population
Rice, D., Nudell, N., Habrat, D., Smith, J., & Ernest, E. (2016). Resuscitation DOI: 10.1016/j.resuscitation.2016.02.013
Free Full Text from Resuscitation.
–
[2] Return of consciousness during ongoing cardiopulmonary resuscitation: A systematic review.
Olaussen A, Shepherd M, Nehme Z, Smith K, Bernard S, Mitra B.
Resuscitation. 2015 Jan;86:44-8. doi: 10.1016/j.resuscitation.2014.10.017. Epub 2014 Nov 4. Review.
PMID: 25447435
–
[3] Anxiety and depression among out-of-hospital cardiac arrest survivors.
Lilja G, Nilsson G, Nielsen N, Friberg H, Hassager C, Koopmans M, Kuiper M, Martini A, Mellinghoff J, Pelosi P, Wanscher M, Wise MP, Östman I, Cronberg T.
Resuscitation. 2015 Dec;97:68-75. doi: 10.1016/j.resuscitation.2015.09.389. Epub 2015 Oct 9.
PMID: 26433116
–
Rice, D., Nudell, N., Habrat, D., Smith, J., & Ernest, E. (2016). CPR induced consciousness: It’s time for sedation protocols for this growing population Resuscitation DOI: 10.1016/j.resuscitation.2016.02.013
–
Olaussen A, Shepherd M, Nehme Z, Smith K, Bernard S, & Mitra B (2015). Return of consciousness during ongoing cardiopulmonary resuscitation: A systematic review. Resuscitation, 86, 44-8 PMID: 25447435
–
Lilja G, Nilsson G, Nielsen N, Friberg H, Hassager C, Koopmans M, Kuiper M, Martini A, Mellinghoff J, Pelosi P, Wanscher M, Wise MP, Östman I, & Cronberg T (2015). Anxiety and depression among out-of-hospital cardiac arrest survivors. Resuscitation, 97, 68-75 PMID: 26433116
.



I have had two arrest patients in recent memory begin growling and moving their limbs during high quality CPR. Whether or not they were aware of their surroundings, I could not say. But my impression of one of them was that he reacted to the pain of defibrillation by suddenly growling louder. That patient actually had a ROSC and was able to tell us his name before he rearrested, during the move to the truck, and never came back.
He may have benefited from Ketamine. Honestly the thought didn’t even cross my mind. More than anything I wish I had told him to say goodbye/I love you to his family during his brief period of consciousness. I appreciate your article and will consider sedation when encounter this situation again.
I have been wanting to make an introduction and elaborate on this a little more for explanation. I finally can. As the lead author of the letter to the editor you commented on I want to first thank you for your comments.
The problem with LTEs is that they are confined to only 500 words making it very difficult to clarify without losing “The Take Home Message.” This LTE was adapted from a full body article which I am pleased to say will be released in the British Paramedic Journal this August or September.
In it, we go into much greater depth as to our rationale and why. I think it will help your readers.
On one point however, there needs to be clarification about the percentages out of Olaussen’s article. Most have skimmed it and felt our reporting of 39% was inaccurate as Olaussen’s article was much lower. This is not the case and you have to read his entire article to understand it.
“Some degree of consciousness” was seen in up to 39% of the patients who had ROSC. However, Olaussen for study purposes had a two phase interview process to eliminate those that had vague memories or responded to painful stimuli. The patients reported were only those who were FULLY awake and could communicate with the CPR team.
The point of our letter and concern as an EMS medical director is this…should fully awake be the threshold to determine whether we need to manage a painful situation?
In Nebraska DHS, we felt that we had to treat CPR almost as a surgical procedure. No one would think it ethical if a patient were in the OR and grunting or groaning during the procedure. These are symptoms of an awareness of pain….even if the patient cannot verbalize it.
So…is the population increasing? Well actually we believe it is…but again it is a bit of a numbers game. Let me explain. Do we think the rate (percentage of those who experience “something” during CPR) is rising? No. But the total numbers of patients who do are. Remember….not every rescue service in America or UK are dialed in to high quality CPR.
When Nebraska adopted a referendum on supporting high quality CPR across our entire state….we saw the bump. Rates are similar but as more paramedics do this…more paramedics will see this. Get the idea?
So that brings me to my last point about our letter (and I do hope you will at least read the full article when it comes out). You are absolutely correct there are no large studies looking at this. For obvious reasons. That being said we had a moral and ethical dilemma. If someone wakes up during CPR do we manage the problem now or do we wait until there are large studies available proving which method might be best? To a physician, we do take that oath that we will “do no harm.” We don’t know (yet) whether sedating with Ketamine has unrecognized risk. But we do know for absolute assuredness that waking up and feeling the pain of CPR is doing harm. Pain has cardiovascular stress implications.
So at least for now…we researched this humbly and carefully to suggest a way to manage it beyond the quick Versed and Midazolam response which we believe might actually cause harm.
All of this being said, that is why I am thankful you decided to post your thoughts. Our article was never intended to be the end of a discussion but rather the very beginning of one. We humbly recognize the limitations of what we had to pen but felt compelled our words had to be stated as scientifically as possible.
Through your posts, comments from paramedics, physicians, and others, we hope this will spark interest in some pig labs or other studies to begin to unravel what drugs might be better suited. Based on published pharmacologic literature, ketamine is the best choice….for today.
When the full article covering these points comes out, I will gladly send you the link.
Kind Regards,
Don Rice, M.D.
Technical Consultant, Nebraska Dept. of HHS, Office of EMS
Adjunct Assistant Professor to Dr. Ernest, University of Nebraska Medical Center, Department of Emergency Medicine
SInce we have introduced HP CPR (with Lucas) I personally have seen 2 of these cases, and know of a handful more. What was once the stuff of urban legend is now reality. In both of my cases sedation and or paralysis was required to continue resuscitation, with benzos and succs.
I think we can agree that completely removing all sympathetic tone in this critical patient population is probably not a good idea. Yes, there is little research on this topic. But this is fringe of resuscitation and a new unexpected consequence of high-performance CPR. I agree with others that we need some guidance, and in the absence of evidence the presence of a basic understanding of medicine must fill in the gaps until that research occurs. Simply standing around with our hands in our pockets waiting for the research, or worse, performing treatments based on ill-fitting protocols (i.e. standard RSI/post intubation sedation) that have a reasonable chance of making things worse.
In my humble opinion, the nebraska protocol may be a good place to start, until research fills in the gaps. Of course , since there is no real money to be made on this research, I am no holding my breath that it will be done in a timely fashion.