In Ethics, Research, and IRBs – Part I, I wrote about the way the different classifications are used to suggest what amount of evidence supports different treatment recommendations. The size of the treatment effect is categorized as Class I through Class III, focusing on Class IIb. Those are also broken down by Levels – LOE A, LOE B, and LOE C. Using the AHA Levels of Evidence. LOE = Level Of Evidence.
–
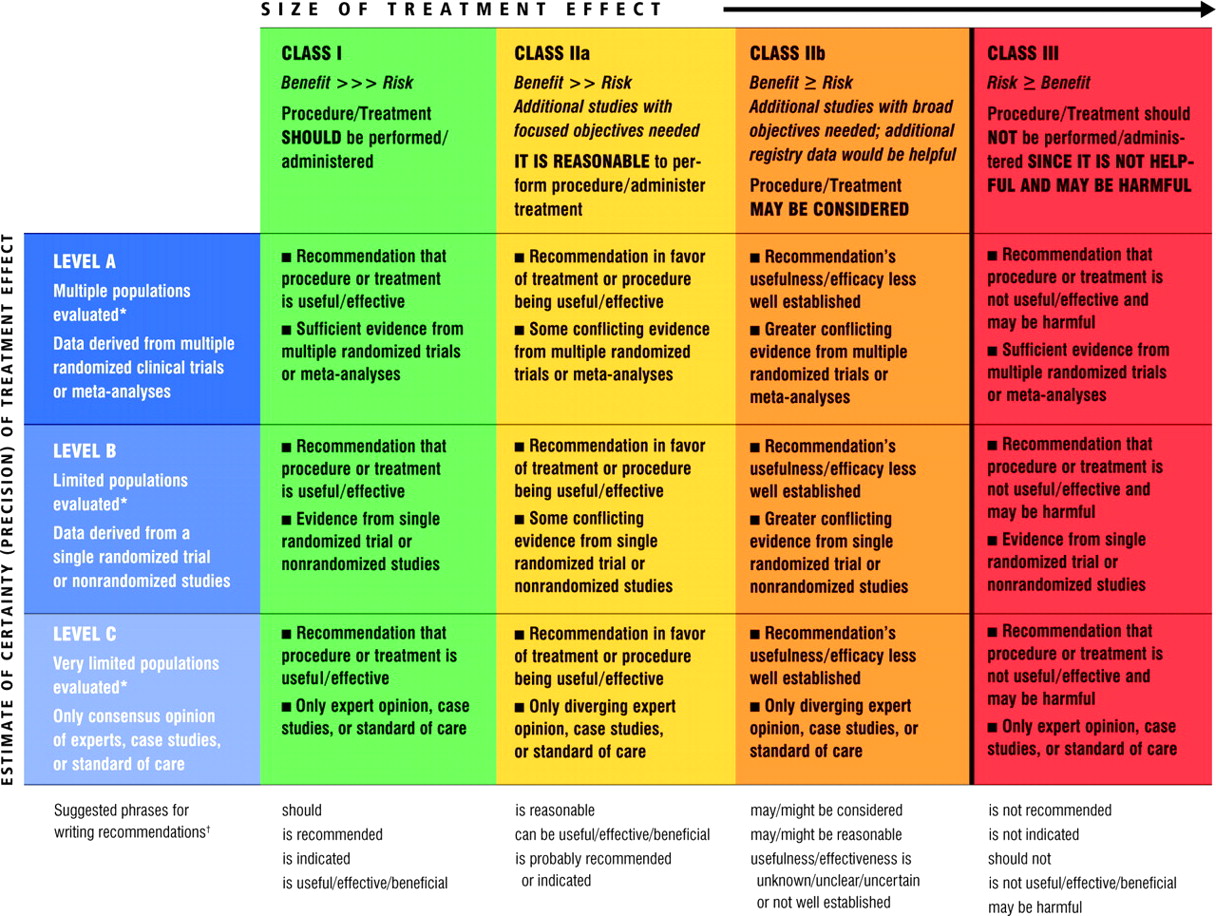
* Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations, such as gender, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use. A recommendation with Level of Evidence B or C does not imply that the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Even though randomized trials are not available, there may be a very clear clinical consensus that a particular test or therapy is useful or effective.
† In 2003, the ACCF/AHA Task Force on Practice Guidelines developed a list of suggested phrases to use when writing recommendations. All guideline recommendations have been written in full sentences that express a complete thought, such that a recommendation, even if separated and presented apart from the rest of the document (including headings above sets of recommendations), would still convey the full intent of the recommendation. It is hoped that this will increase readers’ comprehension of the guidelines and will allow queries at the individual recommendation level.[1]
Click on the image to make it bigger.
The farther to the left and higher on the chart, the better the evidence supporting the treatment and the greater the effect of treatment.
The farther to the right and the lower on the chart, the more laughable worse the evidence supporting the treatment and the less likely there is any beneficial effect of the treatment.
–
That’s nice, but how do we apply this to real treatments?
Let’s look at epinephrine, or any other vasopressor, for cardiac arrest.
When VF/pulseless VT persists after at least 1 shock and a 2-minute CPR period, a vasopressor can be given with the primary goal of increasing myocardial blood flow during CPR and achieving ROSC (see “Medications for Arrest Rhythms” below for dosing) (Class IIb, LOE A).[2]
Class IIb, so the Size of the treatment effect is tiny.
LOE A (Level Of Evidence A), so the Estimate of certainty (precision) of the treatment effect is large.
A large certainty that the treatment effect is tiny.
–
To be continued in Ethics, Research, and IRBs – Part III
–
Footnotes:
–
[1] Table 4. AHA Levels of Evidence
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Part 2: Evidence Evaluation and Management of Potential or Perceived Conflicts of Interest
Free Full Text Article with links to Free Full Text PDF download
–
[2] Drug Therapy in VF/Pulseless VT
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Part 8: Adult Advanced Cardiovascular Life Support
Rhythm-Based Management of Cardiac Arrest
Free Full Text Article with links to Free Full Text PDF download
.



[…] in Ethics, Research, and IRBs – Part II and later to be continued in Ethics, Research, and IRBs – Part […]