
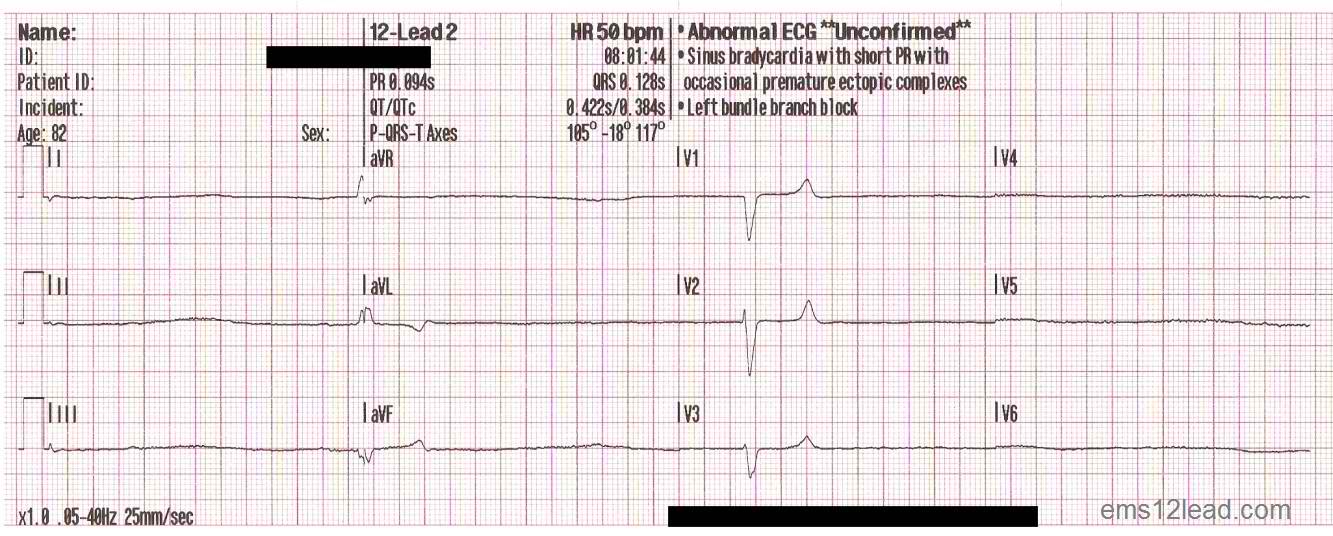
Over at EMS 12 Lead, Tom Bouthillet has a post with this as the rhythm –
Do not click on the image to make it larger. The full sized 12 lead is over there. Go read the post at Tom’s blog, if you haven’t already. Then come back and scroll down to read my comments. Do not skip ahead.
One of the great things about the way Tom posts things is that he makes it interactive. He posts the scenario one day and posts the answer later on. This is a way to get us to think about the question without being able to skip to the end and cheat. This is an excellent way to learn to solve problems and something we should be doing with more of our patients.
We should check back to find out what the diagnosis is for the unusual patients we transported. We can even ask friendly nurses or doctors if there are interesting patients to look at to learn from. If we just transport and forget about the patients, we deprive ourselves of an opportunity to learn. We deprive our patients of better care.
82 Year Old Male CC: Shortness Of Breath
Read this first part.
Think about the condition.
If you want to make it more challenging, limit yourself to a couple of minutes thinking about the rhythm. After all, how much time do you have to sit and ponder on a call?
With this patient, with this rhythm, 2 minutes may be a lot.
When you have given it some thinking, then read the comments. The comments should point out some of the many possibilities that are available, but you may come up with a different way of treating the patient.
After reading the scenario and reading the comments, then read the conclusion. 82 year old male CC: Shortness of breath – Conclusion. Then come back here for some of my thoughts.
*
*
*
*
*
*
Most of you had probably already read Tom’s post before you even got to the beginning of mine.
There is only a little bit of information about medical history, medications, and other information that we want. This is not what we usually get with a scenario, but it is what we often get with real patients.
What do we need to know with this patient?
Age? Social Security Plus is all that I really want to know. If he is 62 or 102, rather than 82, does it matter? Not really. On the paperwork, it matters, but would this patient receive different treatment, if he were 62? No. Would this patient receive different treatment if he were 102? No.
Race? If the guy is white, would we treat him differently? Asian? Indian (from America or from India)? Will any of these affect the treatments we provide?
Smoker? Tom does not include this, but I hear a lot of people ask about this. Will it affect care? Probably not, but it does lead to questions about COPD and related medications.
–
Skin is diaphoretic. Nail beds are bluish. Capillary refill is delayed.
–
How far did I get into the room before I noticed this?
There is no good way to ease into this, so Tom presented the information that we would obtain after we should have noticed the signs of catecholamines being dumped into the body.
My approach to patients is to try to get the big picture first, then look for specifics. How does the patient look in general?
If the answer is, Not bad, then I usually can take it easy and look for reasons to consider the patient unstable. We should always be looking for reasons to change our minds about the patient. An initial assessment is just that – an initial assessment. It becomes a baseline for us to compare later assessments with.
If the answer is, Fixing To Die, then I need to get a few things done quickly, but in a slow and controlled fashion in order to avoid making mistakes. And I need to move the patient safely to the ambulance with the minimum of delays.
What is the minimum information I want? Medications, allergies, medical history, advance directives, when did this begin, has this ever happened before, what have you taken for this, . . . , in this case a blood sugar, pulse oximetry, blood pressure, and 12 lead are indicated on scene.
Look at the vital signs.
RR: ~30 (estimated)
Pulse: 36 Irregular
NIBP: 142/122
SpO2: 88 on RA
On the boxed are of the 12 lead, we can see about 8 seconds of rhythm. There are 4 beats. That works out to 30. The R to R interval (QRS complex to QRS complex or heart beat to heart beat) is irregular. (Late edit 13:49 5/11/2011 – I had written that it is a 9 second strip and that it works out to 36. That would be bad math. It would really be in the upper 20s. However, this is an 8 second strip and that makes the rate about 30. I don’t know why I made that mistake, but I did and I am updating this to the correct numbers.)
More important than the heart rate or the regularity is the strength and equality of the pulses. This is not mentioned, but looking at the NIBP (NonInvasive Blood Pressure) – something is wrong. The systolic reading says Hakuna Matata, but the diastolic says, This is just a random number to be used for entertainment purposes only. We need to compare a manual pressure with the NIBP.
Skin is diaphoretic. Nail beds are bluish. Capillary refill is delayed. . . . and SpO2 of 88 RA (on Room Air)
I do believe the skin signs, because they are telling me about the way the body is responding to what is going on. Is the pulse oximetry accurate? I don’t know and it is not a priority. With cyanotic nail beds and delayed capillary refill, the circulation to the fingers is at least a little bit impaired, so the numbers may be just as random as with the diastolic provided by the NIBP.
Even though the diastolic number looks wrong, we can still trust the systolic pressure, Right?
No.
Yes. It is possible to have a heart rate of 36 and a blood pressure in the normal range.
We are not looking at the big picture, if we are just wondering if those 2 vital signs go together. We should be looking at the skin signs, level of consciousness, and anything else that can give us a clue about perfusion. That is what we are assessing.
Perfusion.
Blood pressure is just a surrogate for perfusion, but if we are looking at an inaccurate number, it isn’t even that.
But back to the rhythm strips. 12 lead #1 shows a rate that looks like it is faster, but the rate listed is slower. Even with the fancy rhythm interpretation software built into the monitor, the indicated heart rate can be a random number generator, too. What is the pulse rate, do the pulses match the QRS beats on the monitor, and what do the pulses feel like?
We don’t know, but the big picture does not look good.
Treatment-wise there are several possibilities.
ASA (Aspirin).
NTG (NiTroGlycerin or GTN GlycerylTriNitrate).
And a bunch of others. Which ones are indicated and why?
I will continue this tomorrow, because there is a lot to discuss. Reading this and figuring out what to do can take much longer than the entire call, so how do we come up with the right treatment? Scenarios that get us to think our way through the possibilities – especially the things that can go wrong.
To be continued in EMS 12 Lead Bradycardia Post – Part II on 5/12/2011.
.



[…] Continuing from Part I. […]