–
Continuing from Part I, Part II, and Part III about the comparative effects of warfarin (Coumadin) and clopidogrel (Plavix) on tICH (traumatic IntraCranial Hemorrhage).
What about the patients with delayed tICH (traumatic IntraCranial Hemorrhage)? There were four cases of delayed tICH.[1] Should this information encourage adoption of the European approach of admitting people for 24 hour observation and repeat CT (Computerized Tomography) scanning?
What would have been the result of a 24 hour observation period with a thousand patients, rather than the paltry 87 (or 97, depending on your ability at math) in the study recommending a 24 hour observation period?[2],[3],[4]
All of these patients were ground-level falls, so from standing, or sitting, or lying on bed. All of these patients had a GCS (Glasgow Coma Scale/Glasgow Coma Score[5]) of 15, which is normal. There does not appear to have been anything alarming about any of these patients, but two of them died – and the information does not provide any clues to identify them while they might have been treated successfully.

Click on images to make them larger.[1]
Delayed tICH patient #2 was admitted without any requirement for 24 hour observation. The delayed tICH was identified on the first day of hospitalization, so this would probably have been picked up by the European protocol.
This patient was probably admitted because the doctor was concerned about something and wanted to observe the patient. The reason for admission and observation is not given.
The patient’s INR (International Normalizated Ratio[6]) was 1.50, which is sub-therapeutic for a patient taking warfarin. Using the INR for guidance would suggest that this patient is not one of the patients at high risk for delayed bleeding due to taking an anti-coagulant. Maybe he has skipped some doses of his medication. Maybe his medication dosing needs to be adjusted.
Delayed tICH patient #2 was discharged home on day 4 with no apparent treatment or complications.
–

Delayed tICH patient #3 was admitted without any requirement for 24 hour observation. The delayed tICH was identified on the seventh day of hospitalization, because of a change in mental status. It is not known if the delayed tICH would have been picked up by the European protocol.
This patient was also probably admitted because the doctor was concerned about something and wanted to observe the patient. The reason for admission and observation is not given.
The patient’s INR was 4.95, which is high, even for a patient taking warfarin. Using the INR for guidance would suggest that this patient is one of the patients at high risk for delayed bleeding due to taking an anti-coagulant. Maybe his medication dosing needs to be adjusted.
Delayed tICH patient #3 improved and was discharged home on day 8 with no apparent treatment or complications.
–

Delayed tICH patient #4 was admitted without any requirement for 24 hour observation. The delayed tICH was identified on the third day of hospitalization, because of a change in mental status. It is not known if the delayed tICH would have been picked up by the European protocol. He was made DNR (Do Not Resuscitate) and died on hospital day without treatment.
This patient was also probably admitted because the doctor was concerned about something and wanted to observe the patient. The reason for admission and observation is not given.
The patient’s INR was 1.90, which is slightly sub-therapeutic for a patient taking warfarin. Using the INR for guidance would suggest that this patient is not one of the patients at high risk for delayed bleeding due to taking an anti-coagulant.
What would it take to prevent his death?
Could anything have prevented his death?
He was already in the hospital when he began to show symptoms.
How many CT scans might have been needed to catch this early?
One every other day?
One every day?
One with each meal?
If this bleed were caught early, would it have made any difference in the outcome?
There is a lot we do not know.
Making rules, based on ignorance, will probably not improve outcomes.
–
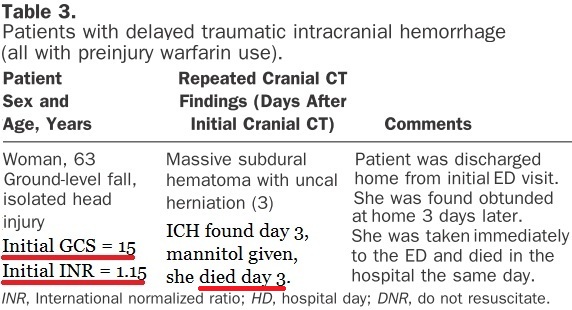
This is the really interesting patient. This is also a very sad case. She was discharged home without admission. The bleed was identified 3 days after the original injury. She was found at home with a level of consciousness described as obtunded, which describes most of the very broad gray area between not fully unresponsive and not fully responsive.
She was taken to the hospital and treated with mannitol (an osmotic diuretic that is used to try to decrease the swelling in the brain) without success. She died that day due to an uncal herniation.

Transtentorial (Uncal) Herniation: (3) Due to the cerebral edema, the uncus of the temporal lobe (medial temporal lobe) herniates downward into the posterior fossa. Central herniation (2) occurs when there is downward pressure centrally and can result in bilateral uncal herniation.[7]
Would a 24 hour observation period have identified this patient?
Was she alone at home?
Did she live alone?
When did she start to have symptoms?
What symptoms did she have?
Could she have recognized these symptoms and called for help?
Was this a sudden onset?
We do not know the answers to any of these questions.
Her INR was 1.15, which is the least likely to raise concerns about any kind of bleeding on warfarin. This level is also sub-therapeutic. Did she start taking extra warfarin because her INR was too low? We don’t know.
Since she was discharged home, we would expect that she leads a somewhat normal life – able to care for herself, or able to be cared for by family, but we do not know any of those circumstances.
What would it take to prevent her death?
Could anything have prevented her death?
If we hospitalize every patient taking an anticoagulant who has a possible head injury, how many patients will have bad outcomes just because of being hospitalized. Unnecessary hospitalization is not benign.
–
Several doctors have suggested that the standard of care needs to be to miss the diagnosis on the first time for several conditions, such as low risk of pulmonary embolus, low risk chest pain. Maybe this should also fall into that category.
The problem is convincing a jury that expects a perfect outcome, no matter how unreasonable that expectation is.
Is it time to initiate medical courts to decide medical issues, rather than have the most medically naive people available make decisions about what is good patient care?
–
Why did the editors decide to make the tiny Menditto study,[2] free for all visitors to their site, but keep this this much larger, very well designed, study behind a paywall? The Menditto study draws broad conclusions from inadequate data. The Menditto study probably should not have been approved for publication, yet it is the featured paper in a prestigious journal.
I expect much better from Annals of Emergency Medicine.
Am I asking too much?
–
Footnotes:
–
[1] Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and preinjury warfarin or clopidogrel use.
Nishijima DK, Offerman SR, Ballard DW, Vinson DR, Chettipally UK, Rauchwerger AS, Reed ME, Holmes JF; Clinical Research in Emergency Services and Treatment (CREST) Network.
Ann Emerg Med. 2012 Jun;59(6):460-468.e7.
PMID: 22626015 [PubMed – in process]
Mp3 of this section of the June 2012 Annals of Emergency Medicine podcast.
–
[2] Management of Minor Head Injury in Patients Receiving Oral Anticoagulant Therapy: A Prospective Study of a 24-Hour Observation Protocol.
Menditto VG, Lucci M, Polonara S, Pomponio G, Gabrielli A.
Ann Emerg Med. 2012 Jan 13. [Epub ahead of print]
PMID: 22244878 [PubMed – as supplied by publisher]
Free Full Text from Annals of Emergency Medicine
–
[3] Observation For Anticoagulated Head Trauma
EM Literature of Note
Radecki
Article
–
[4] This is the Way to Bad Medicine
Rogue Medic
Tue, 24 Jan 2012
Article
–
[5] Glasgow Coma Scale
Wikipedia
Article
–
[6] International Normalizated Ratio
Wikipedia
Article
–
[7] Brain Herniation
CNS Response to Injury
UCSF.edu
Article
–
Nishijima, D., Offerman, S., Ballard, D., Vinson, D., Chettipally, U., Rauchwerger, A., Reed, M., & Holmes, J. (2012). Immediate and Delayed Traumatic Intracranial Hemorrhage in Patients With Head Trauma and Preinjury Warfarin or Clopidogrel Use Annals of Emergency Medicine, 59 (6), 460-2147483647 DOI: 10.1016/j.annemergmed.2012.04.007
–
Menditto, V., Lucci, M., Polonara, S., Pomponio, G., & Gabrielli, A. (2012). Management of Minor Head Injury in Patients Receiving Oral Anticoagulant Therapy: A Prospective Study of a 24-Hour Observation Protocol Annals of Emergency Medicine DOI: 10.1016/j.annemergmed.2011.12.003
.



[…] To be continued in Part IV. […]