On the EMS EduCast, Dr. Ben Abella was on the EMS EduCast discussing the Coursera resuscitation course he taught and the way recent research on therapeutic hypothermia [1]should affect prehospital resuscitation.
During the podcast Dr. Abella states –
I fear, many of the patients that I deal with are much more injured from iscemia reperfusion than the patients in that study. I wonder if the patients in that study just didn’t need that much cooling. You know, if you’re not that sick, you don’t need that much of a dose of medicine, maybe, and if you’re dealing with sicker patients you need more. Now, what I have just said is an unsubstantiated hypothessis. OK. That’s important for people to know. I am not basing that on fact, rather on my experience and opinion.[2]
That is only relevant in some cases.
Sometimes sicker patients require more.
Sometimes sicker patients require less.
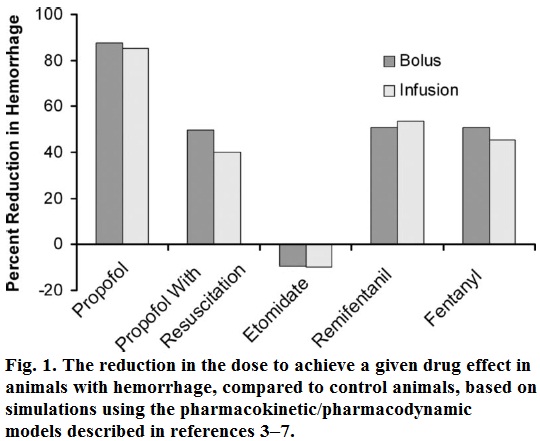
Even with adequate fluid resuscitation, propofol remains substantially more potent in patients with hemorrhage. In marked contrast, the potency of etomidate is nearly unchanged in shock.[3]
According to this, we should only give 10% to 20% of the normal dose of propofol (Diprivan) to the sickest trauma patients, but we should give more than 100% of the normal dose of etomidate (Amidate) to the same patients.
Do the sickest patients require more medicine?
Sometimes yes. Sometimes no.
Pathophysiologists can provide good arguments either way, but pathophysiologists are the philosophers of medicine trying to explain the limited evidence that is available – until more evidence becomes available.
Dr. Abella may be right about starting therapeutic hypothermia prior to transport, but the best available evidence does not support his hypothesis.
Dr. Abella is clear that this is just his hypothesis and he is encouraging more research, because that is the way we find out whether the hypothesis is correct.
–
The EMS EduCast is ending. This is the second to last podcast, from Bill Toon, Greg Friese, and Rob Theriault, but they have nearly 200 podcasts archived to listen to.
–
Footnotes:
–
[1] Targeted temperature management at 33°C versus 36°C after cardiac arrest.
Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise MP, Åneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge JF, Hingston CD, Juffermans NP, Koopmans M, Køber L, Langørgen J, Lilja G, Møller JE, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H; TTM Trial Investigators.
N Engl J Med. 2013 Dec 5;369(23):2197-206. doi: 10.1056/NEJMoa1310519. Epub 2013 Nov 17.
PMID:24237006[PubMed – indexed for MEDLINE]
–
[2] Dr. Ben Abella and the Coursera Cardiac Arrest MOOC: Episode 194
EMS EduCast
December 16, 2013
Podcast page.
–
[3] Shock values.
Shafer SL.
Anesthesiology. 2004 Sep;101(3):567-8. No abstract available.
PMID:15329579[PubMed – indexed for MEDLINE]
Free Full Text from Anesthesiology.
.



Thanks for sharing this episode and your longstanding support of the EMSEduCast.