Also to be posted on ResearchBlogging.org when they relaunch the site.
This is a nice study, which unfortunately ran into problems with enrollment and funding. There are some things that I think should have been done differently.
The doses of chilled IV (IntraVenous) fluid were not weight-based, while the fluid in the human body is weight-based. If midazolam (Versed) was given, the dose was just a single dose of 5 mg, or 2 doses of 5 mg each. The effects of midazolam are much less weight-based, than fluid, but the appropriate way to administer midazolam is to titrate to effect. Even if administering 10 mg of midazolam produces the desired effect in 80%, or 90%, of patients, that can still leave a significant portion inadequately sedated. The goal of TTM (Targeted Temperature Management) may be defeated by the movement of an even mildly agitated patient.
Would another drug, such as ketamine, be more appropriate? How much does use of midazolam affect the use of pressors to counter the vasodilatory effects of midazolam? Unlike other sedatives, ketamine does not seem to produce vasodilation and/or depress cardiac activity. The midazolam was only mentioned in the description of the study interventions and only described as being given to prevent shivering, so the dose may be adequate, but there is only the one mention in the entire paper.
The fluid administration was shown to be different with a p value of <0.0001. The difference is only 170 ml (5 3/4 oz), so it is a distinction described as significant by p value, but it does not appear to be a significant difference in any way that would affect patients. The SD (Standard Deviation - how much variability exists in about 2/3 of patients) is the same as the amount of fluid given to the control group and 2 3/4 times the amount of the difference. In other words, there was a lot of overlap in the volumes administered to the patients in the two groups. While the p value of <0.0001 suggests confidence in the results being due to change only one time in 10,000, that is misleading.
Total fluid infused was not documented for 98 (35%) patients who received Prehospital Cooling and 121 (40%) control patients.[1]
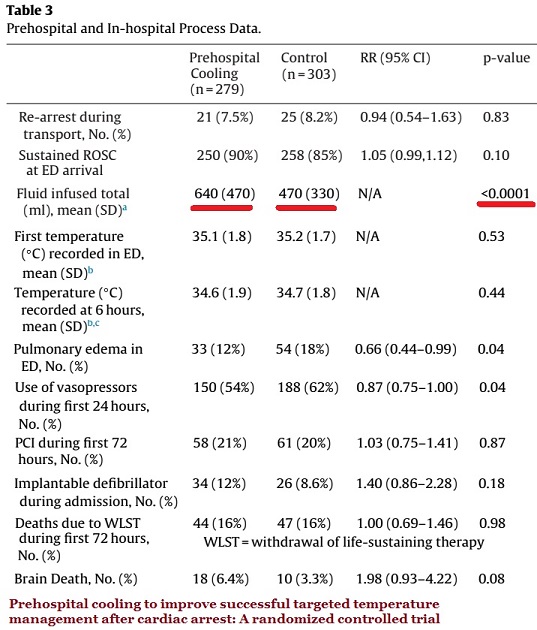
The raw data on the volumes is not included, nor is the shape of the graph of distribution of the volumes, but it looks as if 20%, or 30%, of the control group may have received more fluid that the intervention group – and then there are the more than 35% of patients without documentation of fluid volumes.
Since the amount of difference is small, it does not seem to matter, but the intervention group was forcing the chilled fluid into the patients with pressure bags, so why so little difference between the groups?
How long does it take to administer 170 ml of chilled IV fluid by pressure infusion? Does it take longer than it takes to get from the ambulance to the hospital stretcher?
That is just a statistical oddity that is not going to affect outcomes.
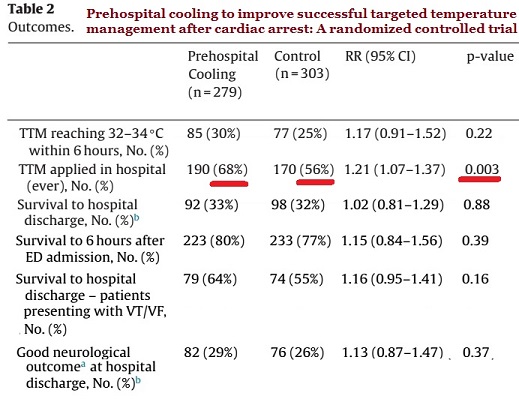
The next may be the true the significant finding of the study.
Patients in the prehospital cooling group were more likely to (ever) receive TTM in hospital [190 (68%) vs 170 (56%); RR 1.21, p = 0.003] than patients in the control group.[1]
TTM (Targeted Temperature Management) is the new term for therapeutic hypothermia, which has been shown to be effective.
If not, why not?
Across all studies that used conventional cooling methods rather than no cooling (three studies; 383 participants), we found a 30% survival benefit (RR 1.32, 95% CI 1.10 to 1.65). The quality of the evidence was moderate.[2]
With no difference in the rhythms of the control group and the intervention group, why the difference in the rate of TTM in the hospital?
Will this be similar to the case of waveform capnography? EMS ended up pressuring many/some EDs to begin to use EtCO2 on all intubated patients. This was a change from the previous, much too common, ED practice of complaining about and pulling at the EtCO2 tubing, because it was an unknown item that was in the way.
EMS should not need to encourage the ED to provide better care, especially about treatments/assessments that originated as in-hospital treatments/assessments. It should be the reverse.
There is an excellent review of TTM research at Life In The Fast Lane.[3]
–
Footnotes:
–
[1] Prehospital cooling to improve successful targeted temperature management after cardiac arrest: A randomized controlled trial.
Scales DC, Cheskes S, Verbeek PR, Pinto R, Austin D, Brooks SC, Dainty KN, Goncharenko K, Mamdani M, Thorpe KE, Morrison LJ; Strategies for Post-Arrest Care SPARC Network.
Resuscitation. 2017 Dec;121:187-194. doi: 10.1016/j.resuscitation.2017.10.002. Epub 2017 Oct 5.
PMID: 28988962
Free Full text Article from Resuscitation.
–
[2] Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation.
Arrich J, Holzer M, Havel C, Müllner M, Herkner H.
Cochrane Database Syst Rev. 2016 Feb 15;2:CD004128. doi: 10.1002/14651858.CD004128.pub4. Review.
PMID: 26878327
–
[3] Targeted temperature management (TTM) after cardiac arrest
Life In The Fast Lane
Chris Nickson
Reviewed and revised Aug 1, 2017 @ 7:07 pm
Article
–
Scales DC, Cheskes S, Verbeek PR, Pinto R, Austin D, Brooks SC, Dainty KN, Goncharenko K, Mamdani M, Thorpe KE, Morrison LJ, & Strategies for Post-Arrest Care SPARC Network (2017). Prehospital cooling to improve successful targeted temperature management after cardiac arrest: A randomized controlled trial Resuscitation, 121 (December), 187-194 : PMID: 28988962
–
Arrich J, Holzer M, Havel C, Müllner M, & Herkner H (2016). Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation Cochrane Database Syst Rev : PMID: 26878327
.



I saw a study at least 5 years ago the simple maltose will open the blood/brain barrier after 20 mins or so. Couldn’t you quickly re-perfuse the brain by administering that simple sugar, instead of the 50% dextrose currently called for ?