I showed the problems with amiodarone for both live patients and dead patients in Part I. The higher the quality of the evidence, the less the evidence supports the use of amiodarone on humans.
Amiodarone is all sales pitch and no medical benefit, but Dr. Kudenchuk keeps trying to spin the results like an acupuncturist, when the evidence clearly does not support Dr. Kudenchuk’s claims.[1]
What else should be de-emphasized?
Obviously, adrenaline (epinephrine in non-Commonwealth countries) for cardiac arrest. As the quality of the epinephrine research has improved, the claims of supposed benefits have disappeared.[2], [3]
Now, the goalposts have shifted, again, and the claims are that some other dosing is safe and effective, even though the evidence to support these claims does not exist. This is alternative medicine. This is dishonest. This is experimenting on patients without any kind of ethical approval, or collection of data, or anything else that would accompany a true experiment. We are learning that we are very good at lying to ourselves, but we knew that.
Eventually, we may be claiming that we have not studied what happens when we stand on one leg while giving epinephrine.
How can we possibly stop using adrenaline if we have not proven that it doesn’t work when standing on one leg? How can we refuse to provide this one legged hope to patients?
We are sorry for what we did to your _______, but we consider justifying doing something harmful, based on low quality evidence and even lower quality excuses, to be more important than the outcomes of our patients. If we don’t throw in the kitchen sink, how can we claim that we did everything we could for to your _______?
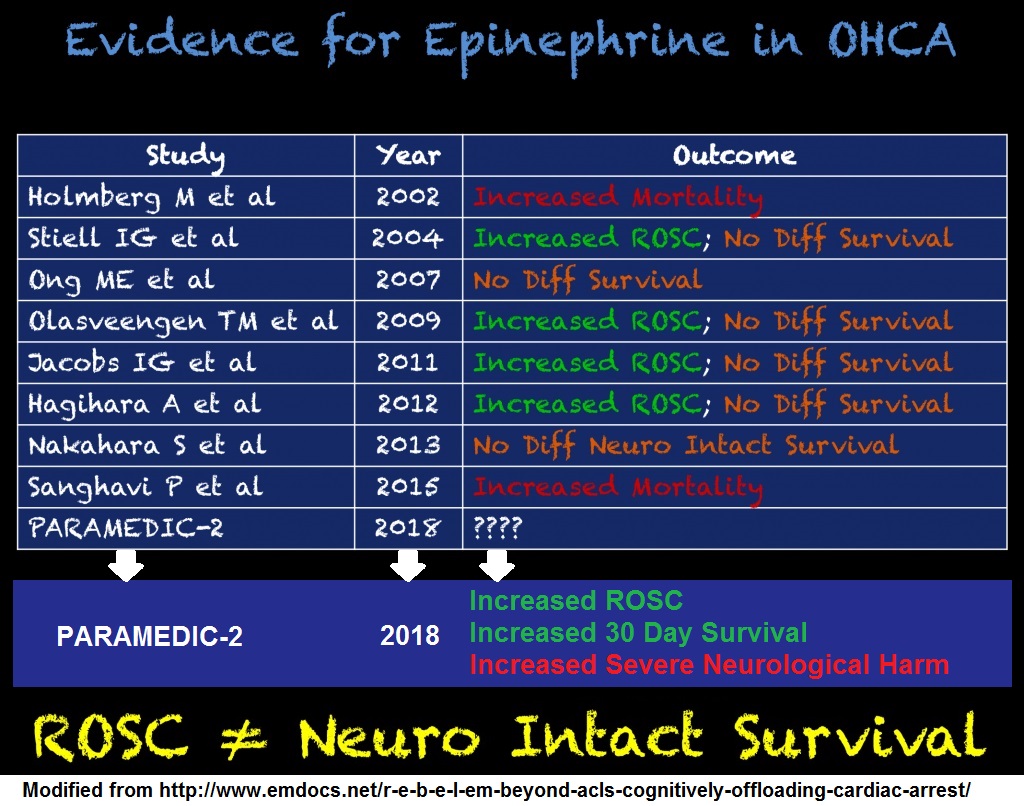
Click on the image to make it larger.
I modified the original to add the outcomes reported by PARAMEDIC2. Severe neurological impairment is the wording from the conclusion, but that would not fit. If you think that harm is not an accurate synonym for impairment, you may be dangerous to patients.
Source of original – R.E.B.E.L. EM – Beyond ACLS: Cognitively Offloading During a Cardiac Arrest
If the next revision of ACLS/ILCOR (Advanced Cardiac Life Support/International Liaison Committee on Resuscitation) does not state that epinephrine/adrenaline should be limited to use in high quality research, it will be encouraging abuse of patients.
This is alternative medicine. This is not medicine.
The difference is that real medicine relies on valid evidence that it works, while alternative medicine relies on marketing strategies and misinformation.
Do you want to be treated by someone who can tell the difference between these approaches?
Medicine requires doing what is best for the patient.
Alternative medicine requires doing what makes the guru look best, so that the guru can keep making sales.
The doctors promoting this unethical approach do not appear to be ashamed of what they are doing, but they keep making excuses. We need to make it clear that their excuses are not ethical.
To all of the doctors claiming that a drip works. Demonstrate that you are ethical and competent. Show that what you are doing improves outcomes that matter to patients, in a high quality study, or stop.
If doctors won’t do that, maybe we should add DNA (Do Not Amio) and DNE (Do Not Epi) to our list of advance directives, for those who do not think that resuscitation to a come, where sepsis and aspiration pneumonia are what we aspire to.
–
Footnotes:
–
[1] Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Cardiac Arrest.
Kudenchuk PJ, Brown SP, Daya M, Rea T, Nichol G, Morrison LJ, Leroux B, Vaillancourt C, Wittwer L, Callaway CW, Christenson J, Egan D, Ornato JP, Weisfeldt ML, Stiell IG, Idris AH, Aufderheide TP, Dunford JV, Colella MR, Vilke GM, Brienza AM, Desvigne-Nickens P, Gray PC, Gray R, Seals N, Straight R, Dorian P; Resuscitation Outcomes Consortium Investigators.
N Engl J Med. 2016 May 5;374(18):1711-22. doi: 10.1056/NEJMoa1514204. Epub 2016 Apr 4.
PMID: 27043165
CONCLUSIONS Overall, neither amiodarone nor lidocaine resulted in a significantly higher rate of survival or favorable neurologic outcome than the rate with placebo among patients with out-of-hospital cardiac arrest due to initial shock-refractory ventricular fibrillation or pulseless ventricular tachycardia.
Here are some comments from Dr. Kudenchuk, which contradict the conclusion of Dr. Kudenchuk’s study:
This trial shows that amiodarone and lidocaine offer hope for bringing patients back to life and into the hospital after cardiac arrest,” said principal study author Peter Kudenchuk, M.D.
This trial shows that amiodarone and lidocaine offer no hope for outcomes that matter to patients.
Importantly, there was a significant improvement in survival to hospital discharge with either drug when the cardiac arrest was bystander-witnessed.”
There is no truth to Dr. Kudenchuk’s claim. This is what the authors of the study actually wrote:
We observed an interaction of treatment with the witnessed status of out-of-hospital cardiac arrest, which is often taken as a surrogate for early recognition of cardiac arrest, a short interval between the patient’s collapse from cardiac arrest and the initiation of treatment, and a greater likelihood of therapeutic responsiveness. Though prespecified, this subgroup analysis was performed in the context of an insignificant difference for the overall analysis, and the P value for heterogeneity in this subgroup analysis was not adjusted for the number of subgroup comparisons. Nonetheless, the suggestion that survival was improved by drug treatment in patients with witnessed out-of-hospital cardiac arrest, without evidence of harm in those with unwitnessed arrest, merits thoughtful consideration.
The best that can be stated about these drugs is that if the researchers used a large enough study, they might be able to find a statistically significant result – or the researchers may demonstrate that this was just another example of a statistically insignificant run of luck, which means nothing and is just as likely to have gone the other way.
A run of heads in a row, while flipping a coin is a reason to examine the coin for bias, but if no bias is found, it is expected to be just what is expected to happen in a large number of coin flips. A lack of understanding of coincidence leads to faulty conclusions.
The difference in outcomes, that Dr. Kudenchuk claims is significant, not statistically significant.
Does Dr. Kudenchuk not understand the way research works or does Dr. Kudenchuk have some unstated motive for distorting the results? It appears that the New England Journal of Medicine refused to publish the conclusion that Dr. Kudenchuk wanted, so Dr. Kudenchuk is using more gullible people to spread his misinformation.
Go ahead and read the full paper, which is available from NEJM here.
Also read Dr. Kudenchuk’s press release, which misrepresents the results of Dr. Kudenchuk’s study. You would think that Dr. Kudenchuk would know better.
Antiarrhythmic drugs found beneficial when used by EMS treating cardiac arrest
NHLBI NEWS|News Release
April 4, 2016, 9:00 AM EDT
Press Release
I have nothing to hide. I want you to look all of the evidence.
Dr. Kudenchuk is Misrepresenting ALPS as ‘Significant’
Tue, 12 Apr 2016
Rogue Medic
Article
Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Cardiac Arrest
Mon, 04 Apr 2016
Rogue Medic
Article
–
[2] Effect of adrenaline on survival in out-of-hospital cardiac arrest: A randomised double-blind placebo-controlled trial
Jacobs IG, Finn JC, Jelinek GA, Oxer HF, Thompson PL.
Resuscitation. 2011 Sep;82(9):1138-43. Epub 2011 Jul 2.
PMID: 21745533 [PubMed – in process]
Free Full Text PDF Download from semanticscholar.org
This study was designed as a multicentre trial involving five ambulance services in Australia and New Zealand and was accordingly powered to detect clinically important treatment effects. Despite having obtained approvals for the study from Institutional Ethics Committees, Crown Law and Guardianship Boards, the concerns of being involved in a trial in which the unproven “standard of care” was being withheld prevented four of the five ambulance services from participating.
In addition adverse press reports questioning the ethics of conducting this trial, which subsequently led to the involvement of politicians, further heightened these concerns. Despite the clearly demonstrated existence of clinical equipoise for adrenaline in cardiac arrest it remained impossible to change the decision not to participate.
The results do not show an improvement in the any outcome that matters to patients.
CONCLUSION: Patients receiving adrenaline during cardiac arrest had no statistically significant improvement in the primary outcome of survival to hospital discharge although there was a significantly improved likelihood of achieving ROSC.
–
[3] A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest.
Perkins GD, Ji C, Deakin CD, Quinn T, Nolan JP, Scomparin C, Regan S, Long J, Slowther A, Pocock H, Black JJM, Moore F, Fothergill RT, Rees N, O’Shea L, Docherty M, Gunson I, Han K, Charlton K, Finn J, Petrou S, Stallard N, Gates S, Lall R; PARAMEDIC2 Collaborators.
N Engl J Med. 2018 Jul 18. doi: 10.1056/NEJMoa1806842. [Epub ahead of print]
PMID: 30021076
It appears that the full text of PARAMEDIC2 is no longer available for free from NEJM, but there is the option of registering for 3 free papers a month (Register for 3 FREE subscriber-only articles each month.) in a red pop-up banner at the bottom of the page.
Once again, the results do not show an improvement in the any outcome that matters to patients.
CONCLUSIONS: In adults with out-of-hospital cardiac arrest, the use of epinephrine resulted in a significantly higher rate of 30-day survival than the use of placebo, but there was no significant between-group difference in the rate of a favorable neurologic outcome because more survivors had severe neurologic impairment in the epinephrine group.
.


Subscribe to RogueMedic.com