
The Skeptics’ Guide to Emergency Medicine should be on your podcast list. The podcasts are short, so there is not much reason to avoid them. This one is 13 minutes.
Valsalva for SVT (SupraVentricular Tachycardia) is supposed to come before medication. At least that is the order of treatments of every EMS SVT protocol I have seen. Since medicine is expected to have more, and more serious, side effects, this is reasonable.
What medicines?
Adenosine has the side effects of –
Cardiovascular
Prolonged asystole, ventricular tachycardia, ventricular fibrillation, transient increase in blood pressure, bradycardia, atrial fibrillation, and Torsade de Pointes
Respiratory
Bronchospasm
Central Nervous System
Seizure activity, including tonic clonic (grand mal) seizures, and loss of consciousness.[1]
It appears to be reasonable to try to avoid those side effects.
Too much of this could become more of a problem than an SVT.

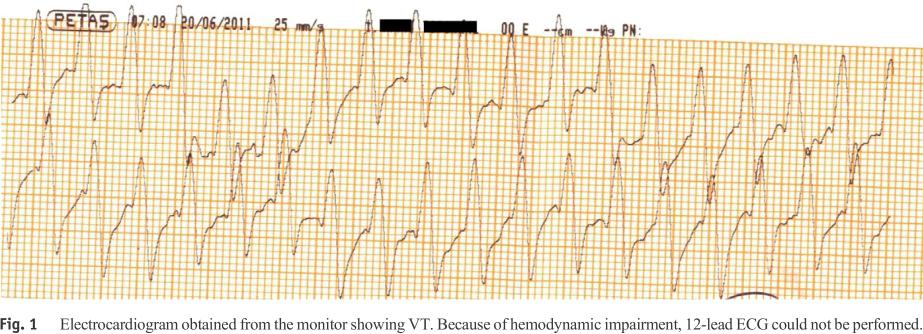
Click on images to make them larger. Image credit.[2] This is not the actual strip, but a strip of an adenosine pause edited to produce more asystole, which I have seen.
The side effect becomes much more of a problem when someone decides to treat the side effect, rather than wait for it to wear off.
We SLAM adenosine in because it wears off quickly. A minute, or two, of asystole is not a problem.
Giving a dose of epinephrine to a patient who had an SVT a minute ago and now has adenosine quickly wearing off – that may be a fatal problem.
But how effective is the Valsalva maneuver (VM)?
The VM is a non-invasive way to convert patients from SVT to sinus.It increases myocardial refractory period by increasing intrathoracic pressure thus stimulating baroreceptors in the aortic arch and carotid bodies Increases vagal tone (parasympathetic).[3]
Here is a big problem with the use of the Valsalva maneuver. It is just one method of attempting to stimulate the vagus nerve.
There are many other methods and they may be more successful. Carotid sinus massage (after auscultation for bruits), facial immersion in ice water (assuring that the airway does not become a problem), bearing down, blowing through a straw (even better may be a swizzle stick), digital circumferential sweep of the anus, coughing, . . . .
There are many ways of activating the vagal nerve, but my favorite is to act as if I have not started an IV before, go very s l o w l y with the insertion of the largest IV catheter I think I can get in the vein, and this has almost always broken the rhythm.
Yes, that is anecdotal, but I have only rarely needed to follow that with medication.
Yes, pain is not a nice thing, but it is much nicer than the side effects listed above.
Bottom Line: There is no standardized methods to perform a VM to terminate uncomplicated SVT that are evidence based.
Clinical Application: VM is a viable technique that is poorly researched for the conversion of SVT and should not be considered essential to attempt prior to chemical cardioversion.[2]
We need better vagal maneuvers.
We need good evidence on what works.
Go read the article and listen to the podcast.
–
Footnotes:
–
[1] ADENOCARD (adenosine) solution
[Astellas Pharma US, Inc.]
DailyMed
FDA Label
–
[2] Atrioventricular Re-entrant Tachycardia
Thumbnail Guide to Congenital Heart Disease
edited version of their adenosine ECG strip
Article
–
[3] SGEM#67: Shock the Monkey Tonight (Valsalva Maneuver for SVT)
Podcast Link: SGEM67
Date: March 23, 2014
Skeptics’ Guide to Emergency Medicine
Article and link to podcast
.
















Subscribe to RogueMedic.com