Some images from the Gathering of Eagles presentation on RAMPART[1] can help to give an idea of what was done to blind EMS to the treatment being given, while minimizing any delay in care that might result from being part of a study. Thank you to Happy Medic for clarifying some of the information not spelled out in the paper.
–
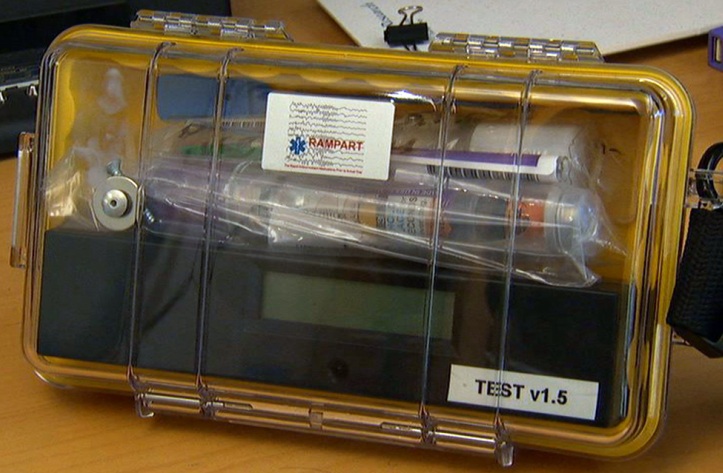
First is the study kit that was used.
For subjects who met the eligibility criteria, the paramedics began the study procedure by opening an instrumented box containing a study drug kit. Each kit contained two color-coded, shrink-wrapped study-drug bundles, one for each dose tier; each bundle consisted of one intramuscular autoinjector (Investigational Midazolam Autoinjector [Meridian Medical Technologies]) and one prefilled intravenous syringe (Carpuject System [Hospira]).[2]
A voice recorder was activated by opening the study box. Paramedics were instructed to record oral statements when intramuscular treatment was administered, when intravenous access was obtained, when the intravenous study drug was administered, when any rescue treatments were given, and when convulsions were observed to stop. Each statement was time-stamped by the study box’s internal clock. Paramedics also stated whether the subject was convulsing on arrival at the emergency department.[1]
–
This is the autoinjector.

–
To assess the weight of the patient for the study, they used a simplified length-based resuscitation tape to measure children to determine whether they were large enough to participate in the trial (at least 13 kg – 28.6 pounds) and whether they would receive the adult dose (over 40 kg – 88 pounds). The low dose was 2 mg lorazepam (Ativan) IV (IntraVenous) or 5 mg midazolam (Versed) IM (Intramuscular). The standard adult dose was 4 mg lorazerpam IV or 10 mg of midazolam IM.

It took me a while to figure out what this was. I initially thought that it was just a label from the side of the study drugs, but when I read it, I realized that this is an image of a full-sized length-based resuscitation tape, just shrunk to fit on the page. That would be about 5 feet long. This is conveniently marked with sections stating DO NOT ENROLL at one end and USE 10 MG DOSE at the other end.
For those who think that randomized placebo controlled studies would interfere with patient care, or delay patient care, this demonstrates that it is pretty easy to get around obstacles and even deliver care faster than outside of the study.
This appears to be an excellent way of designing a randomized double-blind controlled trial.
–
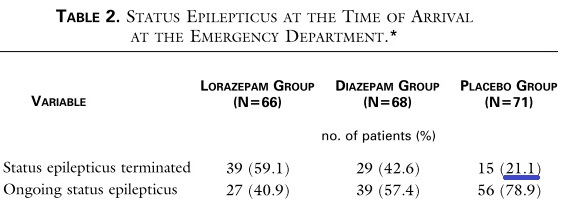
I tried to get some sort of confirmation of the numbers on the IM midazolam group in this last image, but Dr. Jason McMullan does not have them and only the IV lorazepam numbers are in the original paper. I sent a couple of emails to Dr. Robert Silbergleit (the contact person for the paper), but I have not received any response.

The percentage of patients who had their seizures stop prior to starting an IV in the IV lorazepam matches the placebo group from the lorazepam vs. diazepam vs. placebo study.[3]
–
The IV lorazepam group had 21% of the patients not receive IV medication because the seizure stopped without medication.
The placebo group had 21.1% of the seizures stop without any active medication.
The IM midazolam group had 39% of the patients not receive IV medication (just saline since their package included the active midazolam auto-injector) because the seizure stopped before the IV could be started.
The seizures stopped at almost twice the rate that seizures have stopped with placebo treatment. These are just the seizures that stopped before an IV could be started.
–
This study is an excellent example of a prehospital randomized double-blind controlled study that would serve as a great model for a placebo controlled trial of epinephrine.
I have written about this in Intramuscular Midazolam for Seizures – Part I,
Part II,
Part III,
Part IV,
Part V,
Part VI,
Misrepresenting Current Topics in EMS Research from EMS Expo – RAMPART,
and Images from Gathering of Eagles Presentation on RAMPART.
–
Footnotes:
–
[1] Epileptic Fix: Hot-Off-the-Press Results from the RAMPART Trial
Jason T. McMullan, MD (Cincinnati)
Gathering of Eagles
Friday, February 24, 2012
Presentation
–
[2] Intramuscular versus intravenous therapy for prehospital status epilepticus.
Silbergleit R, Durkalski V, Lowenstein D, Conwit R, Pancioli A, Palesch Y, Barsan W; NETT Investigators.
N Engl J Med. 2012 Feb 16;366(7):591-600.
PMID: 22335736
Free Full Text from N Engl J Med.
–
[3] A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus.
Alldredge BK, Gelb AM, Isaacs SM, Corry MD, Allen F, Ulrich S, Gottwald MD, O’Neil N, Neuhaus JM, Segal MR, Lowenstein DH.
N Engl J Med. 2001 Aug 30;345(9):631-7. Erratum in: N Engl J Med 2001 Dec 20;345(25):1860.
PMID: 11547716
Free Full Text from N Engl J Med. with link to PDF Download
.



What’s the “normal” protocol if the patient is convulsing when medics (or first-responders) arrive? Nasal/Buccal Midazolam?
Ollie,
There are many different protocols that can be designed.
The more traditional, less successful way of treating seizures was low dose IV (IntraVenous) diazepam (Valium). If no IV can be started, rectal diazepam is a backup method.
Diazepam, by either method, and even at reasonable doses, is not as successful and not as safe a way to treat seizures, but it is traditional.
As you can see from the study comparing IV lorazepam, IV diazepam, amd IV placebo, only the IV lorazepam worked more than half of the time. The doses were low – 2 mg lorazepam and 5 mg diazepam. The dose could be repeated one time, so this is similar to some old protocols I have had to work with.
.
We have pretty straight forward protocol: If convulsing upon arrival – we are instructed not to even try to get iv-line but to give Midazolam 15mg nas/bucc (for adults, although it’s pretty big dosage imho, for underage the dosage is 0,3mg/kg). If convulsion occurs after iv-line is acquired – lorazepam 2mg up to three times.