.jpg)
Also posted over at Paramedicine 101 (now at EMS Blogs) and at Research Blogging. Go check out the excellent material at these sites.
–
How should this large double-blind, randomized, noninferiority trial comparing IM (IntraMuscular) midazolam (Versed) with IV (IntraVenous) lorazepam (Ativan) affect the way we treat patients with seizures?
–
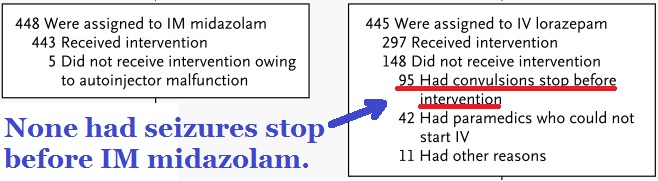
Click on image to make it larger.
21.3% of patients had their seizures stop before they could be given IV lorazepam, while none of the IM midazolam patients had seizures stop before being given medication.
Does that provide a bias toward improved outcomes with IM midazolam?
–
Study Outcomes
The primary outcome was termination of seizures before arrival in the emergency department without the need for the paramedics to provide rescue therapy.[1]
Seizures were absent without rescue therapy on arrival in the emergency department in 329 of 448 subjects assigned to active treatment with intramuscular midazolam (73.4%) and in 282 of 445 assigned to active treatment with intravenous lorazepam (63.4%) (difference, 10 percentage points; 95% confidence interval [CI], 4.0 to 16.1; P<0.001 for noninferiority and P<0.001 for superiority) (Fig. 2).[1]
The patients who had seizures stop without any lorazepam are included in those considered successfully treated.
This is appropriate, since we can expect a similar rate of spontaneous resolution among the patients receiving IM midazolam. The only difference is that those patients will have received the midazolam so quickly that the seizure will not yet have stopped.
Status epilepticus was terminated by the time of arrival at the emergency department in 59.1 percent of patients given lorazepam, 42.6 percent of patients given diazepam, and 21.1 percent of patients given placebo (P=0.001)[2]
Is this a reason to avoid/delay administration of IM midazolam?
No.
The greater risk appears to be to the patients with continuing seizures. The primary benefit of IM midazolam is the rapid administration.
There is no evidence of any harm to the patients who would have their seizures stop without midazolam. There is evidence of harm from delaying/avoiding treatment. Most seizures will stop prior to the arrival of EMS. Delays in treatment should probably only be for those known to have self-limiting seizures and EMS is at the patient’s side in less than 5 minutes.
–
An out-of-hospital complication (hypotension, cardiac dysrhythmia, or respiratory intervention) occurred in 7 (10.6 percent) of the patients treated with lorazepam, 7 (10.3 percent) of the patients treated with diazepam, and 16 (22.5 percent) of the patients given placebo (P=0.08). The most common complication was a change in respiratory status requiring ventilation assistance by bag valve-mask or an attempt at intubation (7 patients given lorazepam, 6 given diazepam, and 11 given placebo).[2]
Those who did not receive benzodiazepines did not do as well as those who did receive benzodiazepines – this includes the most worrisome side effect of benzodiazepines – respiratory compromise. We are not improving outcomes by delaying care or by using low doses.
–
Among subjects admitted to the hospital, the lengths of stay in the intensive care unit and in the hospital did not differ significantly between the groups, but the proportion of subjects admitted was significantly lower (and the proportion discharged from the emergency department was significantly higher) in the intramuscular group than in the intravenous group (P=0.01).[1]
If there is no IV already in place, is there much reason to not use IM midazolam for active seizures?
No.
–
Our data are consistent with the finding that endotracheal intubation is more commonly a sequela of continued seizures than it is an adverse effect of sedation from benzodiazepines.11 [1]
High dose benzodiazepines appear to be more likely to prevent intubation, than to result in intubation. This is something that many medical directors do not seem to have considered.
–
I have written about this in Intramuscular Midazolam for Seizures – Part I,
Part II,
Part III,
Part IV,
Part V,
Part VI,
Misrepresenting Current Topics in EMS Research from EMS Expo – RAMPART,
and Images from Gathering of Eagles Presentation on RAMPART.
–
Footnotes:
–
[1] Intramuscular versus intravenous therapy for prehospital status epilepticus.
Silbergleit R, Durkalski V, Lowenstein D, Conwit R, Pancioli A, Palesch Y, Barsan W; NETT Investigators.
N Engl J Med. 2012 Feb 16;366(7):591-600.
PMID: 22335736
Free Full Text from N Engl J Med.
–
[2] A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus.
Alldredge BK, Gelb AM, Isaacs SM, Corry MD, Allen F, Ulrich S, Gottwald MD, O’Neil N, Neuhaus JM, Segal MR, Lowenstein DH.
N Engl J Med. 2001 Aug 30;345(9):631-7. Erratum in: N Engl J Med 2001 Dec 20;345(25):1860.
PMID: 11547716 [PubMed – indexed for MEDLINE]
Free Full Text from N Engl J Med. with link to PDF Download
–
Silbergleit, R., Durkalski, V., Lowenstein, D., Conwit, R., Pancioli, A., Palesch, Y., & Barsan, W. (2012). Intramuscular versus Intravenous Therapy for Prehospital Status Epilepticus New England Journal of Medicine, 366 (7), 591-600 DOI: 10.1056/NEJMoa1107494
–
Alldredge BK, Gelb AM, Isaacs SM, Corry MD, Allen F, Ulrich S, Gottwald MD, O’Neil N, Neuhaus JM, Segal MR, & Lowenstein DH (2001). A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus. The New England journal of medicine, 345 (9), 631-7 PMID: 11547716
.



The SFFD recently had the opportunity to attend the presentation of this study by the lead researchers from UCSF. They praised the pre-hospital crews on their adherence to the study design and are looking very much forward to using the same locations for further studies.
SFFD enrolled 10% of the study, Detroit had the most, possibly speaking to the socio-economic factors that may impact seizure prevention via healthy lifestyle, medications, screening etc.
HM
Just went back to some materials released by Northern New England Poison Control to us here in the Northeast. In parts of Maine, Bath salts have been a large issue and Midazolam has been looked at as a frontline drug for chemical sedation. NNEPC sited two studies in the Academy of Emergency Med. from 2004 and 2005. Mean time to Sedation by IV for Midazolam was 18 minutes vs. 32 minutes for IV Lorazepam (Nobay et al Acad Emerg Med, 2004). A 2005 study of agitated pts (Martel M et al Acad Emerg Med, 2005) showed 5mg Midazolam vs 5mg Droperidol given IM; the IM Midazolam achieved sedation at 15 minutes vs 30 for other drugs in the study. Just thought these two studies might be of interest to your excellently written articles. Mark
Also should be noted, we dropped 6mg Midazolam IV (2mg initial at about 5-10 minutes, 4mg additional per OMC) per on a seizing pt the other day (Status epilepticus, seizing unknown time, but witnessed by rescue over 15 minutes, given per OMC). The 2mg initial decreased the focal motor activity, but the eyes gave away further ongoing activity. While she did relax and she could no longer maintain an open airway, her respiratory drive continued, and I needed only maintain her head position and suplement her effort with a bag. It was very easy to maintain her sats. It was not until the ER doc RSI’d her, that her effort at spontaneous resps. ended. Mark