Conspiracy theorists come in many flavors of self-deception, but they aren’t really that different from the typical true believer in anything else.
I have been writing about myths that we continue to use as standards of care, in spite of a lack of evidence. These are based on the same belief that are behind the myths being pushed by the 9/11 truthers.
The simplest argument against the truthers is that they blame the Bush administration. The same Bush administration that went to war with Iraq, but did not plant any weapons of mass destruction. Are we supposed to believe that thousands of people would murder thousands of Americans based on where they were when the planes hit, but we could not get a much smaller number of people to frame Saddam Hussein – a guy who is easy to hate.
Not just that, but the conspiracy is supposed to have been carried out in the first year of the first term of President Bush, while the absence of a conspiracy of weapons of mass destruction took place years later, after they had much more time to plan.
I know it because of Screwy Idea X.
Screwy Idea X may be true, may be partially true, may be completely false, or may be completely unrelated.
You have to prove that Screwy Idea X is false.
If Screwy Idea X is false, will it be easy to prove it is false? If it is not easy to prove that Screwy Idea X is false, does that mean that anecdote X is true?

The burden of proof should not be on the person who says, Screwy Idea X is ridiculous.
If you can’t prove that Screwy Idea X is false, that proves that Screwy Idea X is true.
Conspiracy theorists and denialists work on the same principle. There is never enough evidence to prove their idea is wrong.
As long as they can claim that there is a tiny possibility that they are right, that is their proof that they are right.
As long as they can claim that there is a tiny possibility that others are wrong, that is their proof that others are wrong.
Vaccines have saved millions of lives and are probably the safest medications we have, but what if your child has an extremely rare adverse reaction? No, autism is not caused by vaccines.
Alternative medicine is better than real medicine, because of _______. There are many problems with real medicine. I write about the problems – I don’t ignore the problems. Alternative medicine pushers ignore their problems and only criticize the problems of real medicine. Alternative medicine is pretending that an unknown treatment has been kept hidden by a conspiracy of Big Pharma and it really works. Except that the evidence consistently shows that alternative medicine does not perform any better than placebo. Alternative medicine is big business and the business is fraud.
We need to get rid of the prescription and over-the-counter medicines that don’t work. We do not need to add more medicines that don’t work.
Creationism is real and evolution is a lie because of conspiracy X. Even though plenty of religions do not see any conflict between their holy books and evolution. Individual preachers will claim that a literal interpretation is essential, but only when it supports what they preach. If the religious do not agree that 6 Day Creationism is real, and there is no evidence that 6 Day Creationism is real, then why should anyone believe that 6 Day Creationism is science?
We accept the crackpot idea because the true believer is charismatic.
Charisma can cover up a lot of flaws, even flaws as ridiculous as what I have already covered.
In medicine, we have our own true believers.
I know it because of Screwy Idea X.
Bleeding to get rid of bad humors.
Oxygen for myocradial infarction.
Antiarrhythmics for myocardial infarction.
Spinal immobilization for mechanism of injury.
Tourniquets mean amputations.
Ventilation for cardiac arrest.
Rotating tourniquets for CHF (because people with heart failure don’t mind a little amputation).
Furosemide (frusemide, brand name Lasix) moves fluid from the lungs to the kidneys.
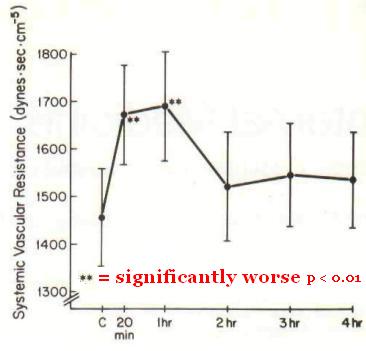
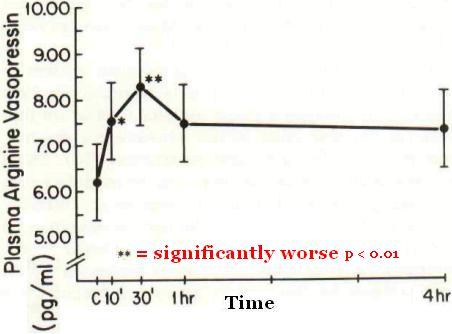
Furosemide causes vasodilation.
If we give pain medicine, the patient will stop breathing.
Even though epinephrine causes heart failure, it is the best solution to a heart that has stopped.
Not just epinephrine for cardiac arrest – vasopressin, norepinephrine, phenylephrine, amiodarone, lidocaine, and magnesium.

The foundation of successful ACLS is high-quality CPR, and, for VF/pulseless VT, attempted defibrillation within minutes of collapse. For victims of witnessed VF arrest, early CPR and rapid defibrillation can significantly increase the chance for survival to hospital discharge.128,–,133 In comparison, other ACLS therapies such as some medications and advanced airways, although associated with an increased rate of ROSC, have not been shown to increase the rate of survival to hospital discharge.31,33,134,–,138 [1]
Maybe the 2015 ACLS Guidelines will be truly evidence-based and will NOT include any medications.
You have to prove that Screwy Idea X is false.
–
Some of the treatments mentioned above have been eliminated, but there are many that continue to be used –
Sunday, I wrote about a doctor claiming that there is a screwy compelling idea that demonstrates that oxygen is good, regardless of the lack of evidence. He also claims that since there is not perfect proof that oxygen is harmful, that is PROOF that oxygen is good.
If it helps just one patient, that justifies killing other patients.
Monday, I wrote about a doctor claiming that there is a screwy compelling idea that demonstrates that spinal immobilization is good, regardless of the lack of evidence. He also claims that since there is not perfect proof that spinal immobilization is harmful, that is PROOF that spinal immobilization is good.
If it helps just one patient, that justifies disabling other patients.
Tuesday, I wrote about a bunch of doctors (the AHA – American Heart Association – and others) claiming that there is a screwy compelling idea that demonstrates that ventilation is good, regardless of the lack of evidence. They also claim that since there is not perfect proof that ventilation is harmful, that is PROOF that ventilation is good.
If it helps just one patient, that justifies preventing the resuscitation of other patients.
I didn’t write anything on Wednesday. I was working on something long for Thursday (even the title was long).
Thursday, I wrote about a bunch of doctors (including the AHA) claiming that there is a screwy compelling idea that demonstrates that tPA is good, regardless of the lack of quality of the evidence. They also claim that since there is not perfect proof that tPA is harmful, that is PROOF that tPA is good hours and hours later.
If it helps just one patient, that justifies causing bleeding in the brains of other patients.
Friday, I wrote about the way the standard of care is perceived. All of these people I mentioned are claiming that their pet treatments, about which they are very biased, should not be affected by any negative evidence and why the evidence in favor of their pet therapy is all that we should pay attention to.
Ignore the flaws of the positive research – assuming there is any positive research. Belief.
Only pay attention to the flaws of the negative research. Willful ignorance.
This is not the way to do what is best for our patients.
If it helps just one patient, that justifies all of the harm to the other patients.
Am I exaggerating?
No, I am just simplifying the excuses for the lack of evidence to support their belief.
If you can’t prove that Screwy Idea X is false, that proves that Screwy Idea X is true.
No.
This is just an example of a logical fallacy.
The argument from ignorance.[2]
–
Footnotes:
–
[1] Overview
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Part 8: Adult Advanced Cardiovascular Life Support
Part 8.2: Management of Cardiac Arrest
Free Full Text from Circulation
–
[2] Argument from ignorance
Wikipedia
Article
.









.jpg)


Subscribe to RogueMedic.com