Also to be posted on ResearchBlogging.org when they relaunch the site.
The results are in from the only completed Adrenaline (Epinephrine in non-Commonwealth countries) vs. Placebo for Cardiac Arrest study.
![]()
Even I overestimated the possibility of benefit of epinephrine.
I had hoped that there would be some evidence to help identify patients who might benefit from epinephrine, but that is not the case.
PARAMEDIC2 (Prehospital Assessment of the Role of Adrenaline: Measuring the Effectiveness of Drug Administration in Cardiac Arrest) compared adrenaline (epinephrine) with placebo in a “randomized, double-blind trial involving 8014 patients with out-of-hospital cardiac arrest”.
More people survived for at least 30 days with epinephrine, which is entirely expected. There has not been any controversy about whether giving epinephrine produces pulses more often than not giving epinephrine. As with amiodarone (Nexterone and Pacerone), the question has been whether we are just filling the ICUs and nursing home beds with comatose patients.
There was no statistical evidence of a modification in treatment effect by such factors as the patient’s age, whether the cardiac arrest was witnessed, whether CPR was performed by a bystander, initial cardiac rhythm, or response time or time to trial-agent administration (Fig. S7 in the Supplementary Appendix). [1]
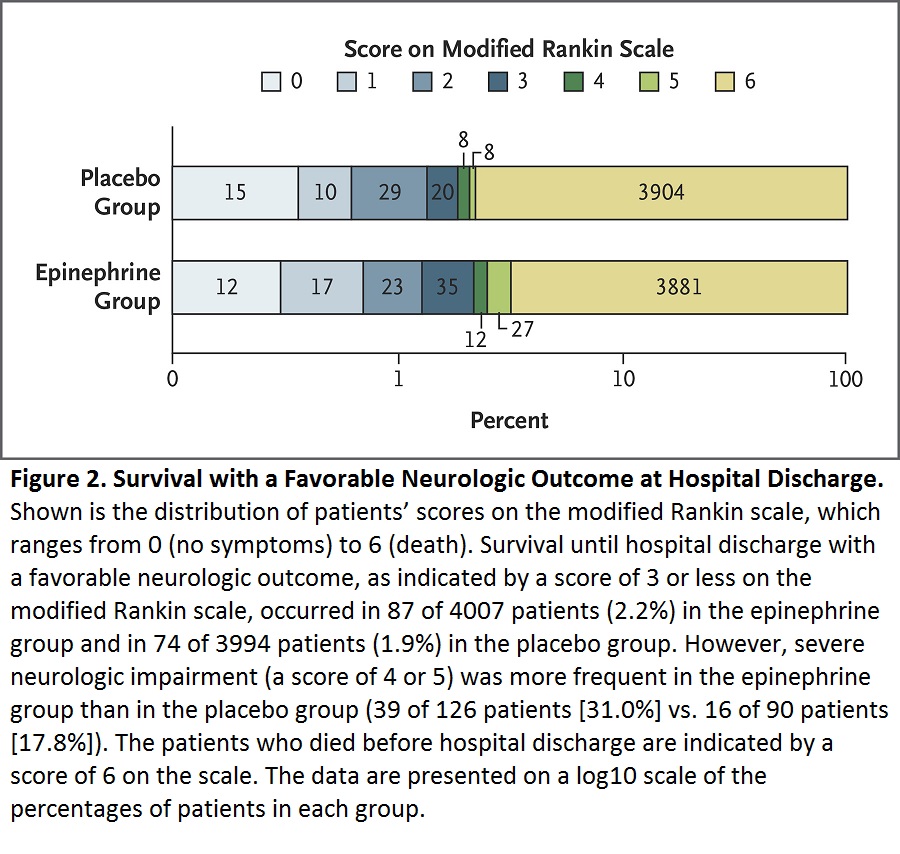
The secondary outcome is what everyone has been much more interested in – what are the neurological outcomes with adrenaline vs. without adrenaline?
The best outcome was no detectable neurological impairment.
the benefits of epinephrine that were identified in our trial are small, since they would result in 1 extra survivor for every 112 patients treated. This number is less than the minimal clinically important difference that has been defined in previous studies.29,30 Among the survivors, almost twice the number in the epinephrine group as in the placebo group had severe neurologic impairment.
Our work with patients and the public before starting the trial (as summarized in the Supplementary Appendix) identified survival with a favorable neurologic outcome to be a higher priority than survival alone. [1]
Click on the image to make it larger.
Are there some patients who will do better with epinephrine than without?
Maybe (I would have written probably, before these results), but we still do not know how to identify those patients.
Is titrating tiny amounts of epinephrine, to observe for response, reasonable? What response would we be looking for? Wat do we do if we observe that response? We have been using epinephrine for over half a century and we still don’t know when to use it, how much to use, or how to identify the patients who might benefit.
I will write more about these results later
We now have evidence that, as with amiodarone, we should only be using epinephrine as part of well controlled trials.
–
Also see –
How Bad is Epinephrine (Adrenaline) for Cardiac Arrest, According to the PARAMEDIC2 Study?
–
Footnotes:
–
[1] A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest.
Perkins GD, Ji C, Deakin CD, Quinn T, Nolan JP, Scomparin C, Regan S, Long J, Slowther A, Pocock H, Black JJM, Moore F, Fothergill RT, Rees N, O’Shea L, Docherty M, Gunson I, Han K, Charlton K, Finn J, Petrou S, Stallard N, Gates S, Lall R; PARAMEDIC2 Collaborators.
N Engl J Med. 2018 Jul 18. doi: 10.1056/NEJMoa1806842. [Epub ahead of print]
PMID: 30021076
All supplementary material is also available at the end of the article at the NEJM site in PDF format –
There is also an editorial, which I have not yet read, by Clifton W. Callaway, M.D., Ph.D., and Michael W. Donnino, M.D. –
Testing Epinephrine for Out-of-Hospital Cardiac Arrest.
Callaway CW, Donnino MW.
N Engl J Med. 2018 Jul 18. doi: 10.1056/NEJMe1808255. [Epub ahead of print] No abstract available.
PMID: 30021078
.













Subscribe to RogueMedic.com