–
Continuing from Part I.
A part of this study that should received more attention is the rate of immediate tICH (traumatic IntraCranial Hemorrhage) among patients taking clopidogrel or warfarin.
5.1% of warfarin (Coumadin) patients had immediate traumatic intracranial hemorrhage.
12.0% of clopidogrel (Plavix) patients had immediate traumatic intracranial hemorrhage.
The sample was from all patients with any kind of head trauma who presented to the participating trauma centers or to the participating community hospitals. From major head trauma transported to a trauma center through to minor head trauma, such as the patient transported to a community hospital because of a nursing home slid out of bed in the dementia unit and might have hit head protocol. This should increase the relevance of this study to emergency physicians in community hospitals and could affect the decisions about where to transport these patients.
More than 60% of patients with immediate traumatic intracranial hemorrhage in both warfarin and clopidogrel cohorts had a normal mental status (GCS score = 15).[1]
Does that mean that tICH is more common with a normal GCS (Glasgow Coma Scale/Score) than with a lower GCS?
No.
Definitely not.
From Table 4, there are 45 tICH patients with a GCS of 15. There are a total of 70 tICH patients. 45/70 = 64.3%.
Only 64.3% of patients with a tICH had a GCS of 15, while the patients with a GCS of 15 made up 87.6% of the patients evaluated for head injury. 3.6% of the warfarin patients with a GCS of 15 had immediate tICH, while 9.2% of the clopidogrel patients with a GCS of 15 had immediate tICH.
Only 12.4% of the patients had a GCS <15, but they made up 35.7% of the cases of tICH.
Suppose we don't require a GCS of 15, but only ≥13. Those with a GCS of 12 or less made up 2.7% of patients, but 15.7% of the cases of tICH. It appears that the lower the GCS, the greater the likelihood of tICH, but a GCS of 15 is not a reason to assume that there is no head injury, especially if the patient is taking clopidogrel.
1/11 clopidogrel patients (GCS of 15 and hit head) will have a bleed vs. 1/28 warfarin (GCS of 15 and hit head) patients. Are the newer drugs better? Will the claimed better than clopidogrel drugs be better at avoiding side effects or will they be better at causing intracranial bleeding from minor injuries? The newer drugs include prasugrel (Effient), ticagrelor (Brilinta), dabigatran (Pradaxa), rivaroxaban (Xarelto), and others.
We don’t know yet, but it would not be reasonable to assume that these drugs will be safer.
–
Should all anticoagulated patients receive a CT scan, regardless of how unremarkable their physical exam?
According to the authors, yes. However, they did not scan every patient. There were 64 patients who did not receive CT scans. This is about 2/3 of the size of the study that claims that these patients should be observed in the hospital for 24 hours, then receive another CT scan.[2]
How reckless was skipping the CT on these apparently uninjured patients?
–
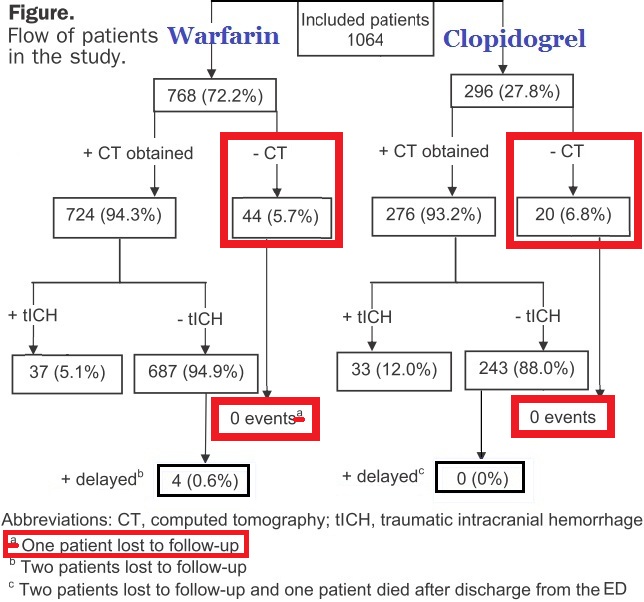
Click on image to make it larger.
–
Zero patients with tICH.
This is from a very small number (64 patients), so it is not good evidence (and the authors do not claim that this is good evidence), but this is almost on a par with numbers in the Menditto study (97 patients).[2] With small numbers, we can come up with answers that satisfy almost any hypothesis.
Is there good evidence for admission and a 24 hour observation period followed by a second CT scan for every anticoagulated patient with any head trauma?
No.
Is there good evidence for a CT scan for every anticoagulated patient with any head trauma?
Yes. Until there is a good way to decide which patients do not need to be scanned. The problem is that there does not appear to be a good substitute for a CT scan – and even the CT scan misses tICH (delayed tICH).
27/70 (38.7%) tICH patients had neurosurgery or died.
How many of them had a GCS of 15?
How many of them had a GCS of ≥13?
–
What was it about these patients that encouraged the doctors to not use a CT scan on the 64 patients who did not receive a CT scan?
We do not know.
When we look at the delayed tICH patients, we will see that there is not an easy way to pick out the slow bleeds from the GCS, INR, mechanism, or anything else.
–
Table 4 shows that those 45 tICH patients are out of 45/870 patients with a GCS of 15. 45/870 is 5.2%. This is from Table 4, out of the total of 1,064 patients, so why do they state elsewhere that there are 932 patients (87.6%) with a GCS of 15? Where are the 62 patients who make up the difference? The footnote states that this is *Based on patients who received a cranial CT scan on initial evaluation after head injury. The conclusion appears to be that 62/64 (96.9%) patients, who did not have a CT scan, did have an initial GCS of 15. That makes sense. 45/870 patients who had a GCS of 15, had a CT scan, and had an immediate tICH.
Normal mental status (GCS = 15) – 932 (87.6%).
752 (70.7%) patients had physical examination findings of head trauma above the clavicles, but only 707 of those patients had CT scans and 50/707 (7.1%) had immediate tICH. 45 patients with physical examination findings of head trauma above the clavicles do not appear to have had a CT scan. 45 (70.3%) of the 64 patients who did not have a CT scan, do appear to have had physical examination findings of head trauma above the clavicles. When reading the results in Table 4, this appears to be the explanation for the differences in the numbers. It would be nice if this were clearer on the first reading of the paper.
–
To be continued in Part III and Part IV.
–
Footnotes:
–
[1] Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and preinjury warfarin or clopidogrel use.
Nishijima DK, Offerman SR, Ballard DW, Vinson DR, Chettipally UK, Rauchwerger AS, Reed ME, Holmes JF; Clinical Research in Emergency Services and Treatment (CREST) Network.
Ann Emerg Med. 2012 Jun;59(6):460-468.e7.
PMID: 22626015 [PubMed – in process]
There is a podcast covering this at Annals of Emergency Medicine. Podcast on this article in Mp3 format.
–
[2] Management of Minor Head Injury in Patients Receiving Oral Anticoagulant Therapy: A Prospective Study of a 24-Hour Observation Protocol.
Menditto VG, Lucci M, Polonara S, Pomponio G, Gabrielli A.
Ann Emerg Med. 2012 Jan 13. [Epub ahead of print]
PMID: 22244878 [PubMed – as supplied by publisher]
Free Full Text from Annals of Emergency Medicine
There is a separate podcast covering this article at Annals of Emergency Medicine. Podcast on this article in Mp3 format.
I covered this in January in This is the Way to Bad Medicine.
–
Menditto, V., Lucci, M., Polonara, S., Pomponio, G., & Gabrielli, A. (2012). Management of Minor Head Injury in Patients Receiving Oral Anticoagulant Therapy: A Prospective Study of a 24-Hour Observation Protocol Annals of Emergency Medicine DOI: 10.1016/j.annemergmed.2011.12.003
–
Nishijima, D., Offerman, S., Ballard, D., Vinson, D., Chettipally, U., Rauchwerger, A., Reed, M., & Holmes, J. (2012). Immediate and Delayed Traumatic Intracranial Hemorrhage in Patients With Head Trauma and Preinjury Warfarin or Clopidogrel Use Annals of Emergency Medicine, 59 (6), 460-2147483647 DOI: 10.1016/j.annemergmed.2012.04.007
.





Subscribe to RogueMedic.com