Big city EMS departments like to brag about how good they are, but are they good?
“If you think about how much progress we’ve made in the last two years, I’m very pleased with the deployment we have now. Are we 100 percent yet? No, but we’re working on it,” Miramontes said. [1]
No sensible person should argue with progress, but –
How bad were things?
How bad are things now?
How much work needs to be done to get to the level of competent?
What are the problems?
If this does not play, it is available at the link in the first footnote.
According to D.C. paramedic Gene Ryan, there has been mismanagement, but according to David A. Miramontes MD, FACEP, NREMT, Assistant Fire Chief, things have dramatically improved. Dr./Asst. Fire Chief Miramontes is management.
Whom should we believe?
“If you’re a burn patient with agonizing pain I could fix that, I could take your pain away, but hopefully you live in the right neighborhood,” Ryan said. “Hopefully it’s the neighborhood that carries that medication, and that’s hit or miss.”
In response, Assistant Fire Chief David Miramontes told News4 control drugs are deployed to more than 90 percent of the department’s units.[1]
Well, morphine and diazepam (Valium) are probably hard to come by, so the problems are to be expected, right?
No.
DCFEMS also carries fentanyl (Sublimaze) and midazolam (Versed) according to their protocols from 2012.[2] Why the failure to provide these basic ALS (Advanced Life Suopport) medications on the ALS ambulances?
Is there any reason why any fire department EMS service should not have excessive amounts of pain medicine on every ALS ambulance? If there is one thing fire departments should be familiar with, it is burns.
Burns mean pain – a lot of pain.
Anyone who has dealt with significant burns knows that more than 100 mg of morphine or more than 1,000 mcg (more than 1 mg) of fentanyl is not an unreasonable dose.
How can a medical director who is also an Asst. Fire Chief tolerate that? Or is the medical director the problem?
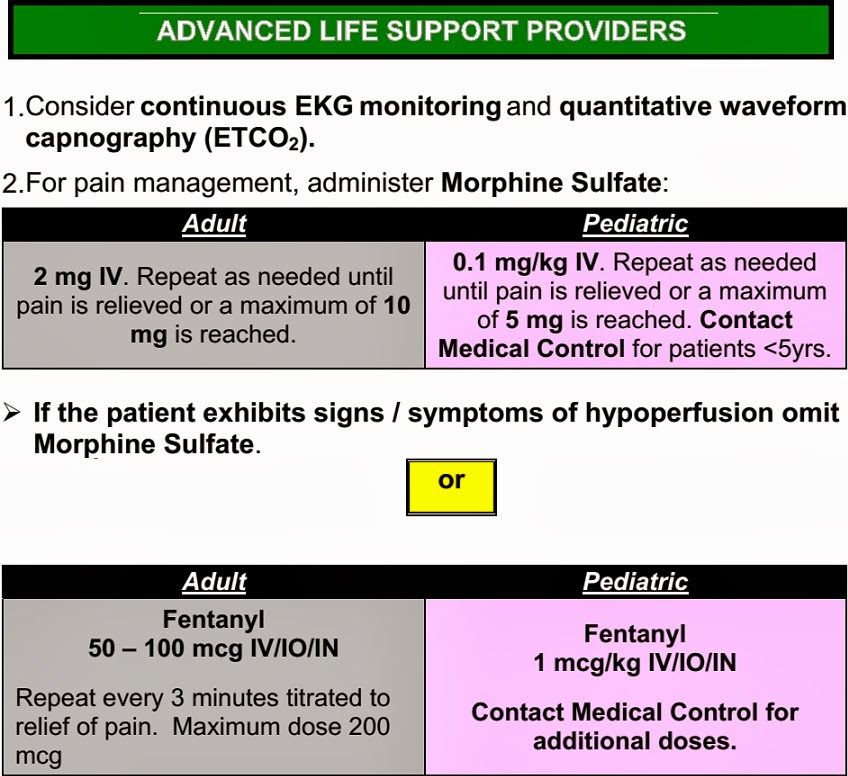
The dose for burns is half of what is permitted for every other painful condition.
What possible legitimate reason is there for not adequately stocking overstocking pain medicine?
Half a year ago, there was a problem with ambulances catching fire and running out of fuel. Management blamed the employees and claimed to be unaware of problems. In other words, management was failing to manage. The job of management is to help the employees to do their job well, not to make excuses.
Fire officials say they are trying to address various problems in the department. They hired a private consultant for $182,000 to audit the fleet after the inspector general found that they had lost track of reserve vehicles, listing many fire engines as ready for duty when they had, in fact, been stripped and sent to scrap yards.
After more than 60 ambulances had mechanical issues last month, including many with broken air conditioning during a heat wave, . . . .[3]
More than 60?
Out of how many ambulances?
Ambulances and Medic Units
- 14 ALS Medic Units
- 25 BLS Ambulances[3]
More than 60 out of 39 in just one month.
Time to replace some ambulances.
But ambulances are expensive. We can’t afford them.

14 Heavy Mobile Equipment Mechanics plus 3 foremen in the top 25 DCFEMS overtime earners.[4]
Maybe the heavy mobile equipment they work on does not include ambulances, but this suggests that there is a problem with the management of equipment. Is the equipment too old. Is the department understaffed? Is there some other reason for these employees being over-represented?
But top fire officials have accused the rank and file of contributing to the breakdowns and staffing shortages through neglect or incompetence,[3]
Our employees are out of control and we are powerless to do anything?
That excuse does not appear to be valid.
DCFEMS has gone through a bunch of medical directors, but adequate stocking of ambulances is still just something to dream about? Is the medical director able to make decisions independently, or is he being not able to exercise authority?
I do not know the answers, but the more people keep failing to fix the problems, the more it looks like DCFEMS needs to be scrapped and remade from scratch with new management. The duct tape is not working.
Mismanagement and retaliation vs. out of control employees?
Management is not making a persuasive case.
–
Footnotes:
–
[1] D.C. Paramedic Plans to Sue Fire Department
By Mark Segraves
Saturday, Feb 22, 2014 | Updated 5:00 AM EST
News4 NBC Washington
Article
–
[2] Emergency Medical Services Manual and Pre-hospital Treatment Protocol
David Miramontes, MD FACEP, Assistant Chief, Medical Director
Kenneth B. Ellerbe, Fire & EMS Chief
Effective Date: September 14th, 2012
Revision Date: September 24th, 2012
Version: 1.1
Page 146/303
Protocols at DC.gov in PDF Download format.
–
[3] Two D.C. ambulances catch fire while on call
By Peter Hermann
Published: August 13, 2013
Washington Post
Article
–
[4] Response to Questions Asked by the Committee for “Fiscal Year 2011 and 2012 Performance Oversight”
Government of the District of Columbia Fire and EMS Department
Council of the District of Columbia
Committee on Public Safety and the Judiciary
Phil Mendelson, Chair
February 3, 2012
Document in PDF Download format.
.





















{kind=link}
{kind=link}
Subscribe to RogueMedic.com